Nickel & Endometriosis: The Metalloestrogen Connection
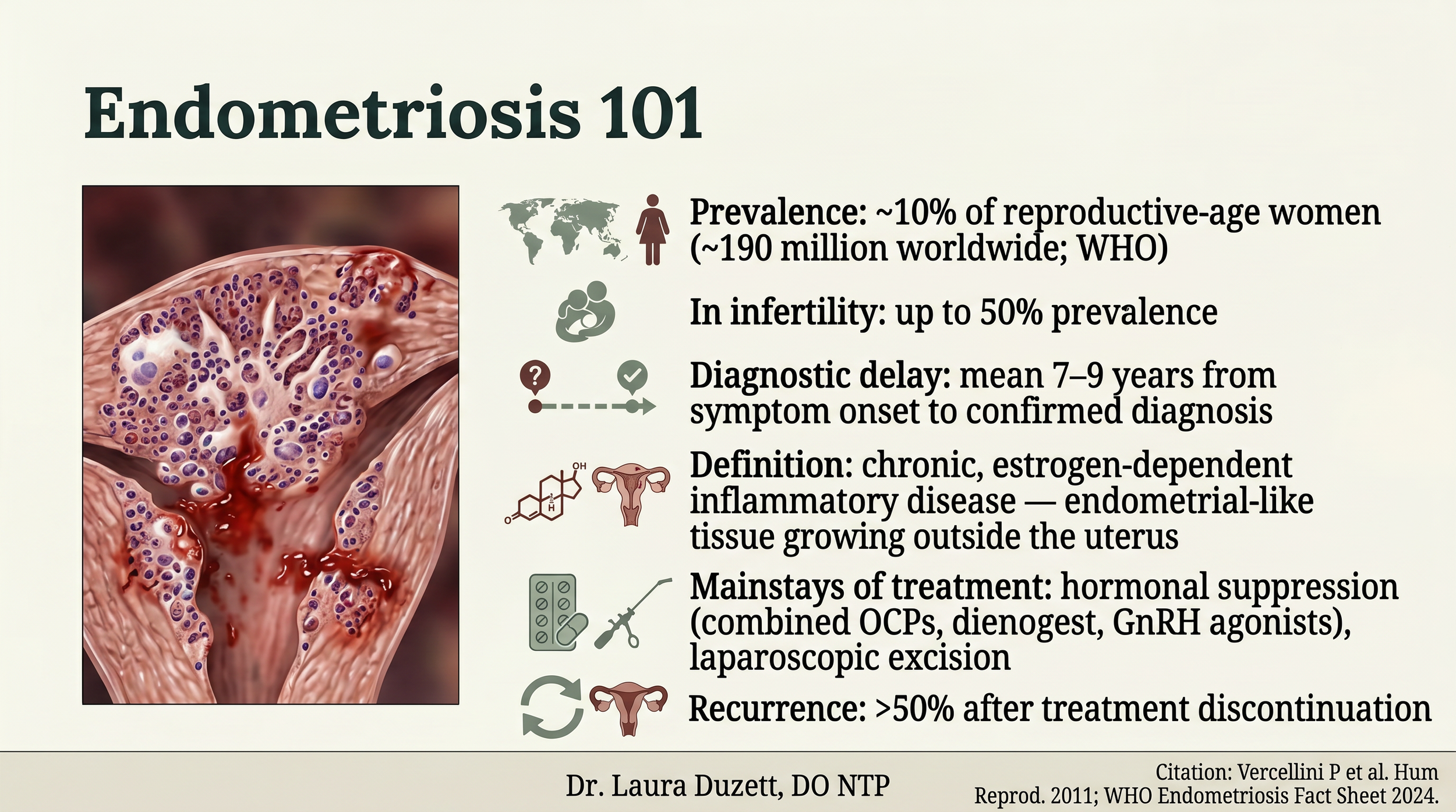
Endometriosis basics
Nickel and Endometriosis: What the Research Actually Shows
If you have endometriosis and you also deal with gut symptoms — IBS-like bloating, reflux, irregular stools, food sensitivities you can't pin down — there's a connection your gynecologist almost certainly hasn't been taught. The research linking nickel hypersensitivity to endometriosis has accumulated quietly across allergy, gastroenterology, immunology, and reproductive endocrinology journals over the last decade, and it has not yet made it into the mainstream gynecology training framework.
This is a long post. I'm going to walk you through the research, the mechanism, and the practical implications — including what we know strongly, what's mechanistically plausible, and what's still hypothesis. The goal is not to convince you that nickel causes your endometriosis. It's to give you the tools to evaluate the evidence for yourself and decide whether a structured low-nickel diet trial belongs in your symptom-management toolkit.
What Your Gynecologist Was Taught About Endometriosis
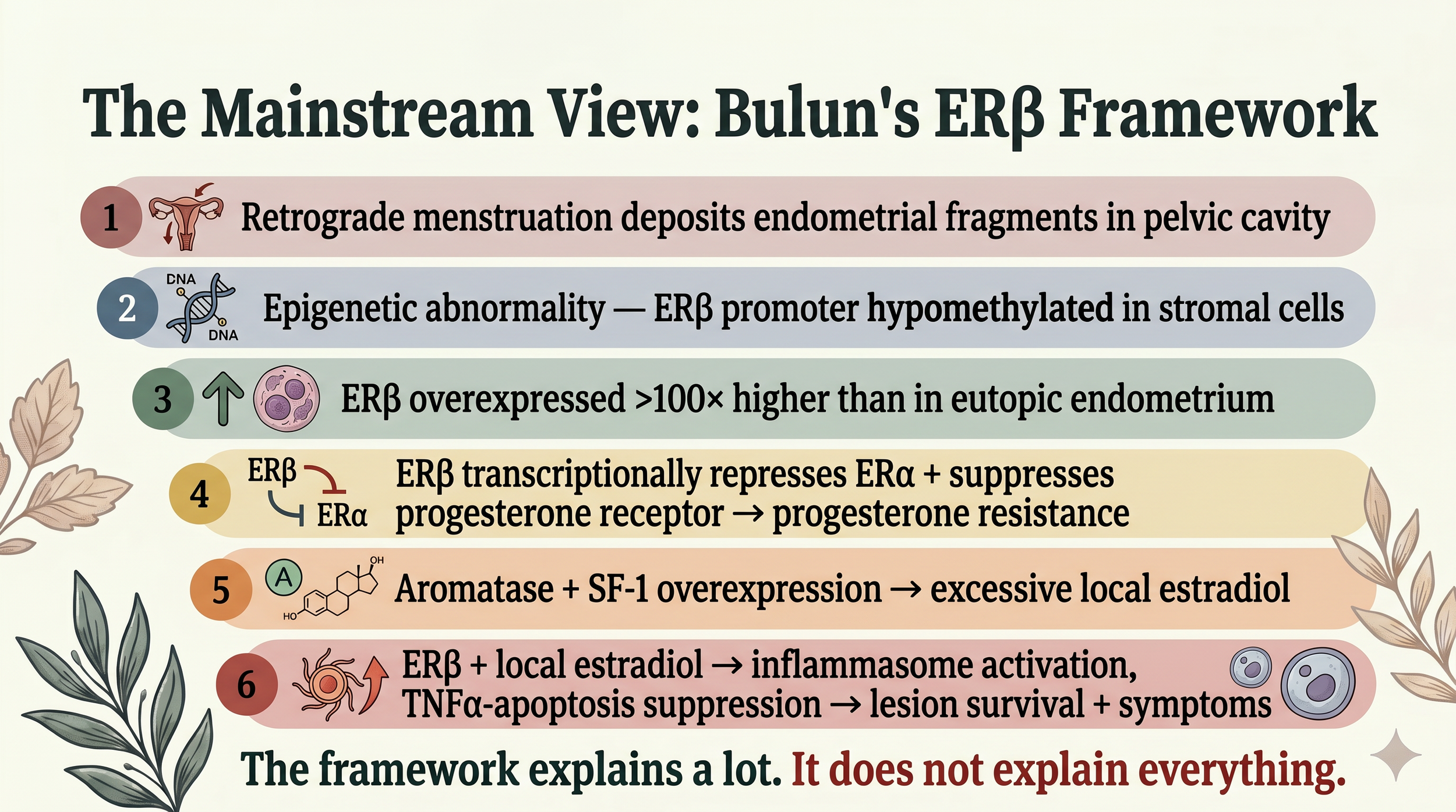
The mainstream framework for endometriosis, most thoroughly synthesized in Bulun and colleagues' 2019 Endocrine Reviews paper, looks roughly like this:
- Retrograde menstruation deposits endometrial fragments into the pelvic cavity (this is necessary, but not sufficient — about 90% of women have some retrograde menstruation, only 10% develop endo).
- Endometriotic stromal cells carry an epigenetic abnormality: the promoter for estrogen receptor beta (ERβ) is hypomethylated, which means the gene is more accessible to transcription.
- ERβ is overexpressed in the resulting lesion stroma — more than 100 times higher than in eutopic endometrium.
- Elevated ERβ transcriptionally represses ERα and suppresses progesterone receptor expression, producing the progesterone resistance that defines the disease.
- Local aromatase and SF-1 overexpression produce excessive local estradiol, which drives the chronic inflammatory and survival signals through ERβ.
This framework is correct as far as it goes. It explains why endometriotic lesions survive instead of clearing, why standard hormonal suppression helps but rarely fixes the problem, and why progesterone resistance is a near-universal feature.
What it does not explain is what causes the methylation defect in the first place. Bulun himself acknowledges this is an open question. The candidate explanations include environmental endocrine disruptors, chronic inflammation, and heavy metals — but no single cause has been identified, and the upstream root remains unresolved.
That open question is where today's research lives.
The mainstream gynecology framework leaves the upstream cause of ERβ overexpression unanswered.
The Story Your Textbook Didn't Tell You: Mast Cells in Lesions
While the mainstream framework focused on stromal cells, parallel research in immunology and reproductive immunology has been documenting something the gynecology textbook hasn't yet integrated: endometriotic lesions have significantly increased mast cell density compared to healthy endometrium. Anaf and colleagues (2006) and Sugamata and colleagues (2005) established this in human tissue. The mast cells in lesions are not bystanders — they are activated, they express estrogen receptors (specifically ERα and the membrane receptor GPR30), and they respond to the locally elevated estradiol in the lesion environment.
When local estradiol activates ERα on mast cells, the cells degranulate — releasing histamine, tryptase, and a cocktail of inflammatory mediators. Tryptase activates PAR2 on sensory nerves, lowering their firing threshold and making the same lesion produce more pain. When local estradiol activates GPR30 on mast cells, the cells release FGF2, which activates FGFR1 on sensory nerves and directly sensitizes pelvic pain perception. A 2023 paper by Xu and colleagues in Frontiers in Immunology demonstrated this end-to-end in a rat model and showed that an FGFR1 inhibitor reversed endometriosis pain.
This is the mechanism that explains why two women with similar lesion stages can have wildly different symptom severity. The lesion is necessary. The mast cell amplifier in the lesion microenvironment is what makes the lesion painful.
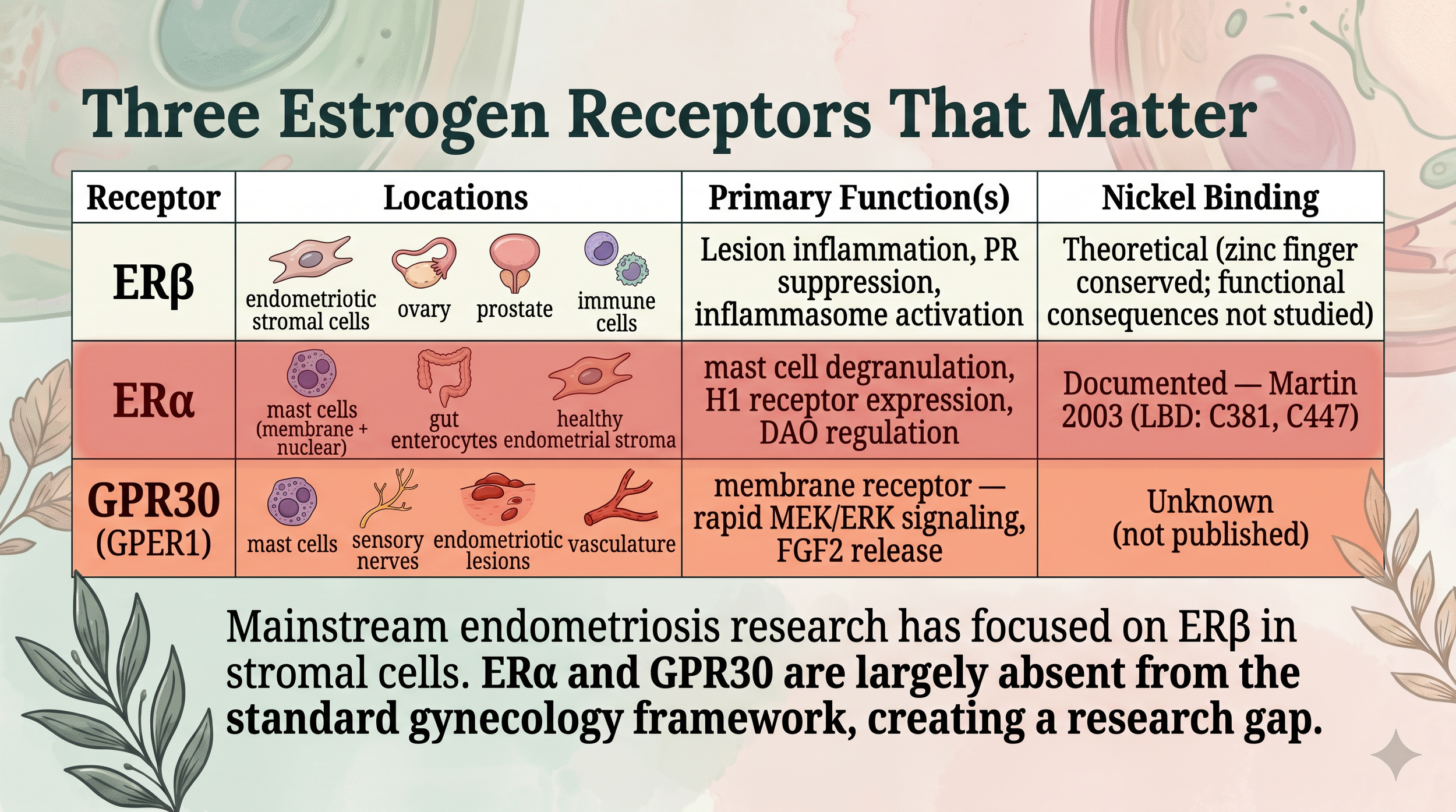
ERα drives mast cells; ERβ drives stromal lesion biology; GPR30 drives pain sensitization. Nickel's documented binding is at ERα.
Where Nickel Comes Into the Picture
Nickel is a metalloestrogen — a term coined by Darbre in 2006 for metals that bind and behave like estrogen at estrogen receptors. Specifically, Martin and colleagues (2003) showed that nickel binds the ligand binding domain of ERα at two specific cysteine residues. In ERα-positive breast cancer cells, nickel mimics estradiol's proliferative effect at about 1000-fold higher concentration than estradiol itself.
The implications for endometriosis become interesting when you stack three findings together.
First, in a Korean nested case-control study of 4,985 women published by Yuk and colleagues in PLoS ONE in 2015, nickel allergy diagnosed years BEFORE endometriosis was associated with 2.5-fold higher odds of being subsequently diagnosed with endo. The temporal direction matters — nickel allergy came first. And the specificity is striking: endometriosis was NOT associated with allergic rhinitis, atopic dermatitis, drug allergy, or broader contact dermatitis. Only nickel-specific allergy.
Second, Silva and colleagues (2013) found that whole blood nickel concentrations were 3.25 times higher in Sri Lankan women with laparoscopically confirmed endometriosis than in similarly-symptomatic but endo-negative controls — and cadmium and lead levels did not differ. Again, the specificity is striking.
Third, and most clinically actionable, Borghini and colleagues (2020) in Nutrients recruited 31 women with endometriosis AND significant gastrointestinal symptoms. Using the oral mucosa patch test (which is more sensitive than the standard skin patch test for systemic forms of nickel hypersensitivity), they found 90.3% of these women were positive for nickel allergic contact mucositis. After three months on a structured low-nickel diet, statistically significant improvement was documented across all measured symptom categories: gastrointestinal, extra-intestinal (including foggy mind), AND gynecological — dysmenorrhea, dyspareunia, and pelvic pain.
Three mandatory caveats apply to Borghini's data. Small sample size. Selection bias (the cohort was specifically recruited for endo + GI symptoms). And single research group. But within that specific clinical population — women with endometriosis and overlapping GI symptoms — this is the strongest published clinical evidence for any dietary intervention.
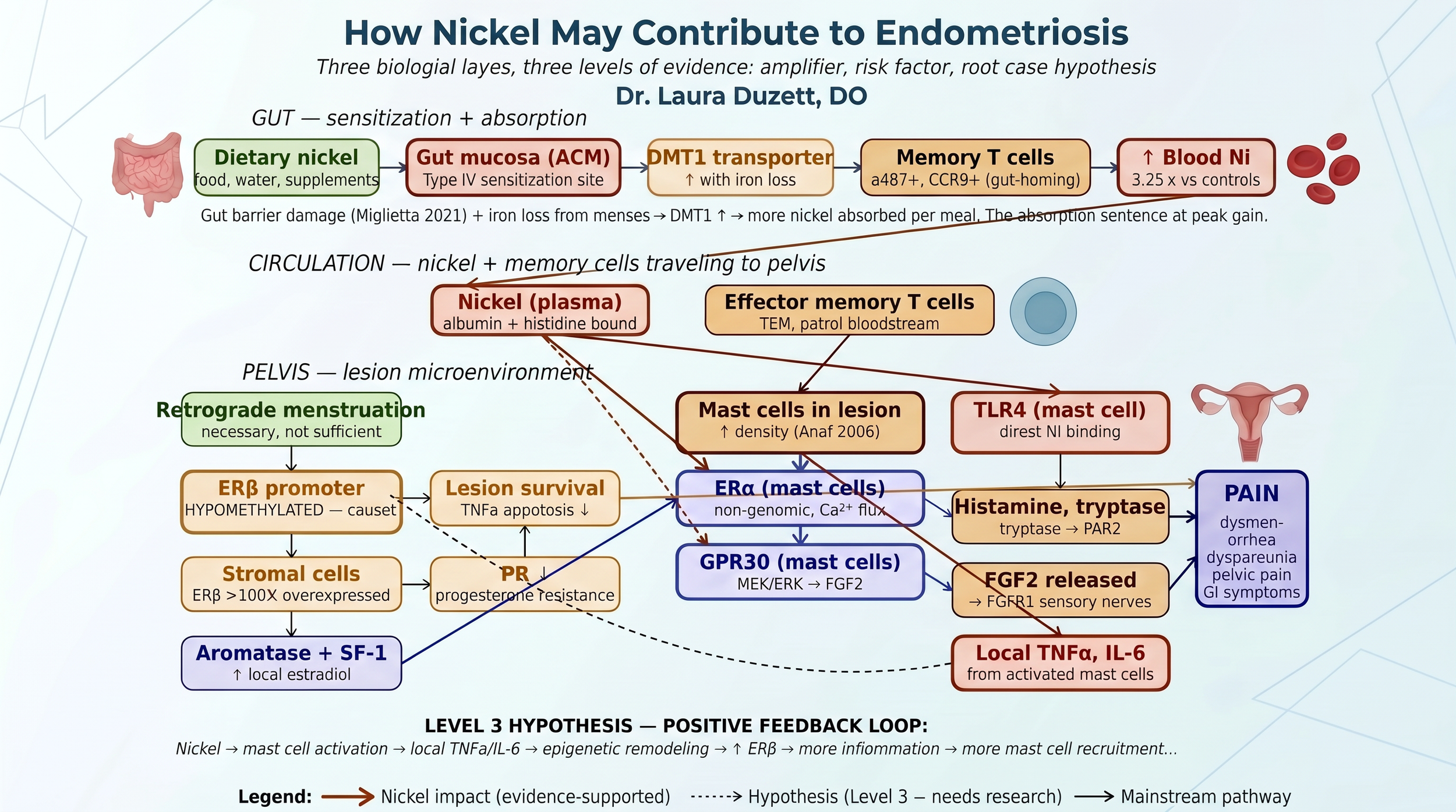
How nickel may fit into endometriosis pathophysiology — three biological layers, three levels of evidence.
How Nickel Reaches the Uterus
Sensitization to nickel does not happen in the endometrium. The endometrium is shed and rebuilt monthly — biologically the wrong tissue for stable Type IV hypersensitivity to develop. Sensitization happens in the skin, the gut mucosa (the dominant route for SNAS), or in regional lymph nodes around implants. Once a person is sensitized, the chain to pelvic tissue is straightforward: dietary nickel is absorbed (more efficiently in SNAS patients because of barrier damage and DMT1 upregulation from menstrual iron loss), enters the bloodstream, and is distributed to highly vascular pelvic tissues — especially endometriotic lesions, which are angiogenic by nature. The mast cells and recruited memory T cells in pelvic tissue do the rest.
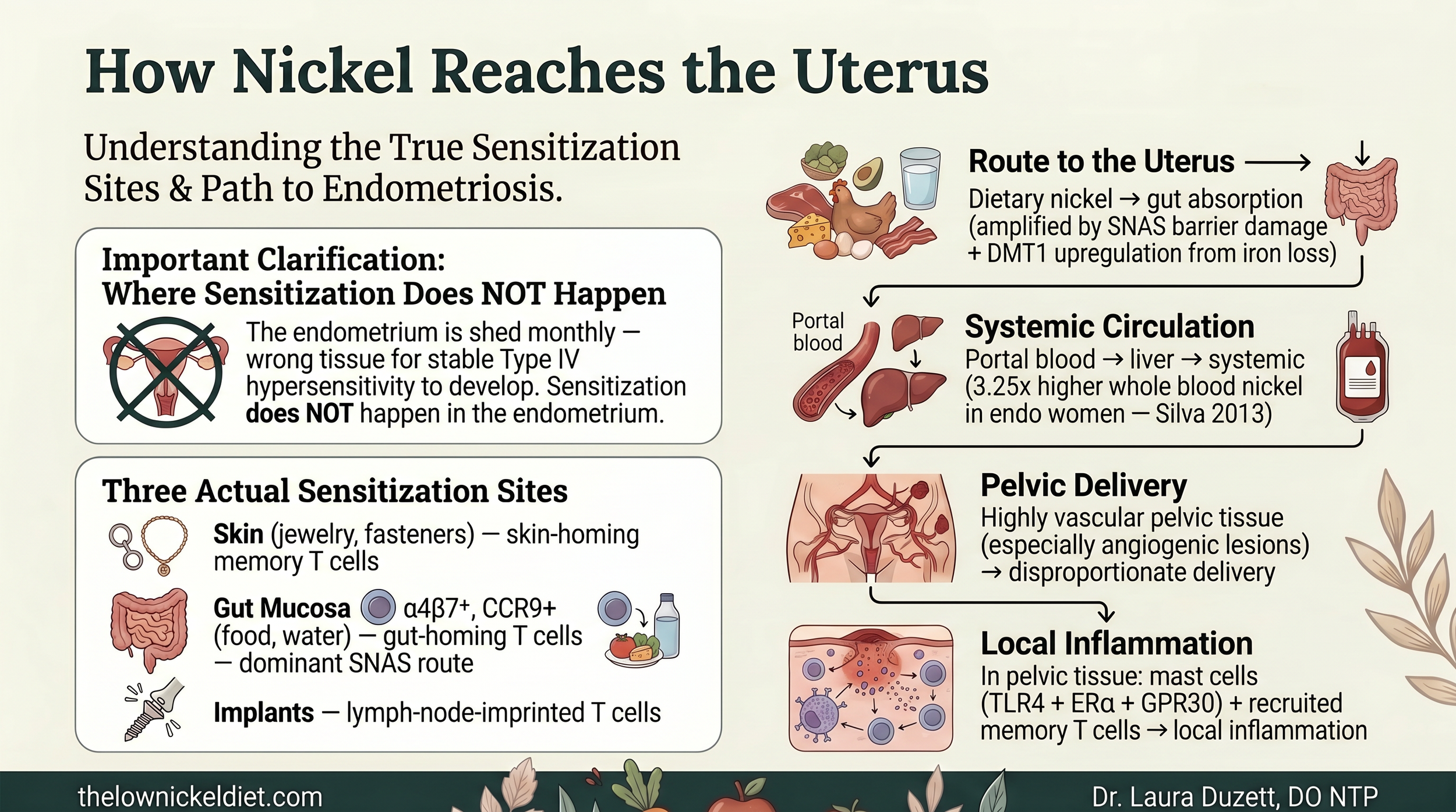
How nickel reaches the uterus in endometriosis: the gut → blood → pelvis chain.
What This Means In Practice
For a woman with endometriosis, the practical implications depend on which symptoms dominate.
If you have endometriosis AND significant gastrointestinal symptoms, a structured 6 to 8 week low-nickel diet trial has the strongest evidence base of any dietary intervention published for this population. The Borghini data shows improvement across all three symptom domains — not just the GI symptoms. The mechanistic explanation is that nickel feeds the mast cell-driven inflammatory amplifier in pelvic tissue, and removing nickel turns that amplifier down.
If your symptoms worsen premenstrually, that pattern is mechanistically consistent with mast cell + histamine amplification through the estrogen-driven pathways. A low-nickel diet plus targeted mast cell stabilization is worth a trial.
If you have comorbid fibromyalgia, MCAS, histamine intolerance, or dyshidrotic eczema — the multi-system SNAS phenotype — the case for addressing nickel becomes stronger because you're addressing one upstream trigger across multiple downstream presentations simultaneously.
The intervention is compatible with current standard endometriosis management. You can do this alongside hormonal suppression, after excision, while on Lupron or dienogest or an OCP. The diet does not shrink lesions and is not a substitute for medical management. It may meaningfully reduce inflammation-driven symptoms.
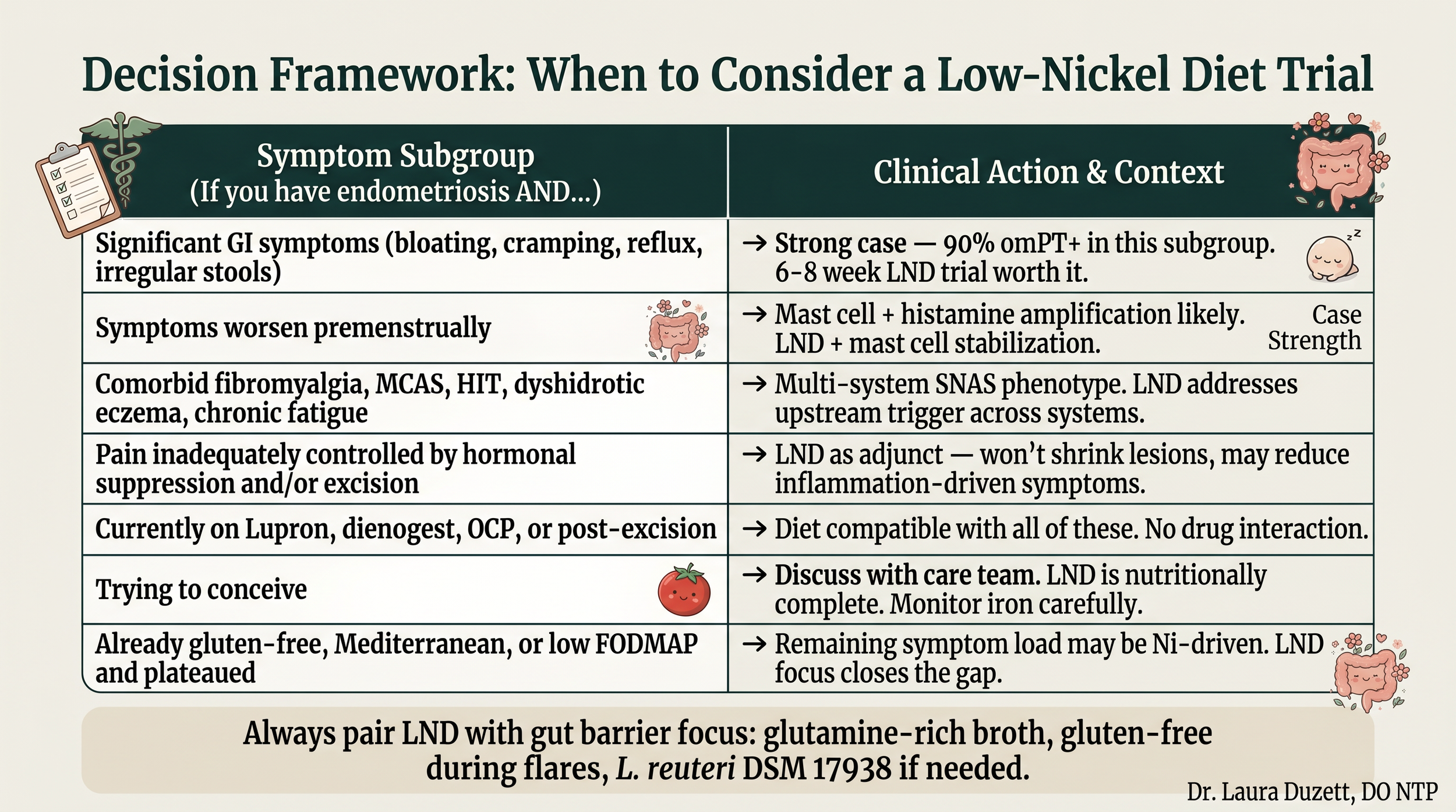
Decision framework: when a low-nickel diet trial is worth considering for endometriosis.
What We Still Need to Prove
Honesty about gaps matters. Borghini's 90.3% is impressive but needs replication in larger, multi-center, controlled trials. Yuk's population data needs validation outside Korea. And the feedback loop hypothesis — that chronic nickel-driven mast cell cytokines may help cause the ERβ promoter hypomethylation that defines the lesion — is mechanistically supportable but has not been directly tested. These are research priorities, not present claims.
What we do have is a coherent, mechanistically grounded explanation for why some women with endometriosis improve dramatically on a low-nickel approach and others see little change. The answer to "is nickel involved in endometriosis?" is not yes or no. It's "yes for a meaningful subset of women, and the only way to know if you're in that subset is to try."
Related Reading
- What is Systemic Nickel Allergy? — the foundational explainer
- Histamine Intolerance and the Nickel Connection — the five-point histamine framework
- Fibromyalgia and Nickel Allergy — the multi-system phenotype
- SNAS Testing — what works, what doesn't
- What is the Low Nickel Diet? — how to actually do it
References
- Borghini R, Porpora MG, Casale R, et al. Irritable Bowel Syndrome-Like Disorders in Endometriosis: Prevalence of Nickel Sensitivity and Effects of a Low-Nickel Diet. Nutrients. 2020;12(2):341. PMID 32012984.
- Yuk JS, Shin JS, Shin JY, et al. Nickel Allergy Is a Risk Factor for Endometriosis. PLoS ONE. 2015;10(10):e0139388. PMID 26439741.
- Silva N, Senanayake H, Waduge V. Elevated levels of whole blood nickel in Sri Lankan women with endometriosis. BMC Res Notes. 2013;6:13. PMID 23317102.
- Bulun SE et al. Endometriosis. Endocr Rev. 2019;40(4):1048-1079. PMID 31074265.
- Xu X et al. GPR30-mediated estrogen pathway in mast cells participates in endometriosis pain. Front Immunol. 2023;14:1106771. PMID 36845134.
- Aquino NB et al. Cadmium and nickel in estrogen receptor signaling. J Environ Sci Health C. 2012;30(3):189-224.
- Schmidt M et al. Crucial role for human TLR4 in nickel contact allergy. Nat Immunol. 2010;11(9):814-819.
- Martin MB et al. Estrogen-like activity of metals in MCF-7 cells. Endocrinology. 2003;144(6):2425-2436.
Disclaimer: This article is for educational purposes only. It is not medical advice. I am Dr. Laura Duzett, DO NTP — a physician and pathology resident, and a Nutritional Therapy Practitioner. I am coaching dietary protocols only, not practicing medicine. Always consult your own care team before making changes to your diet, supplements, or treatment plan. Individual results vary.
If you want to dig deeper into a personalized protocol, the Endometriosis Companion Guide and the printable Doctor's Letter (for your next OB/GYN appointment) live inside