Fibromyalgia and Nickel Allergy: The Mast Cell, Gut, and Mitochondria Connection
Fibromyalgia and Nickel Allergy: The Mast Cell, Gut, and Mitochondria Connection
If you have fibromyalgia, you have probably been told one of two things: it is all in your head, or nobody really knows what causes it. The 2024-2025 peer-reviewed research says both of those statements are wrong.
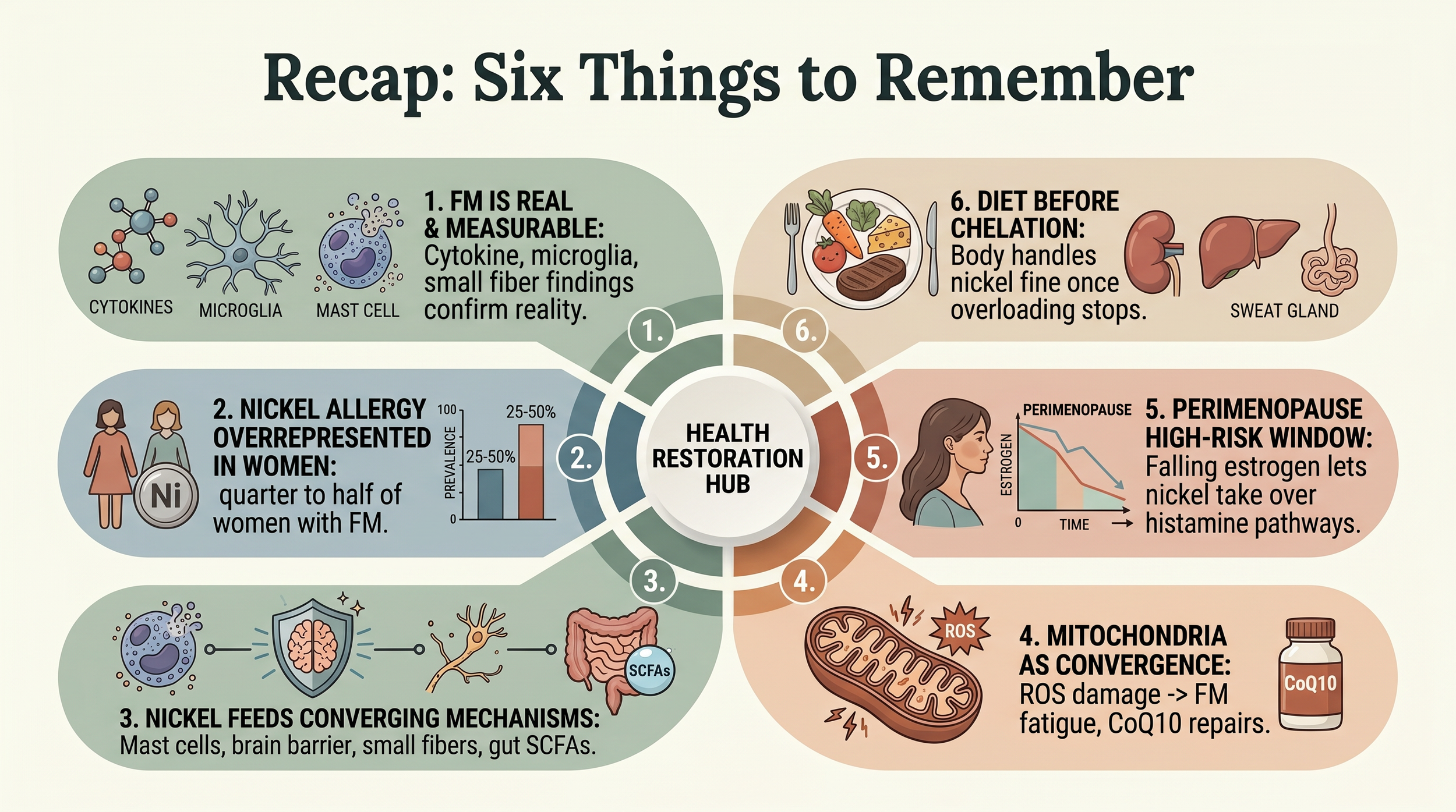
Fibromyalgia is a real biological disease with measurable findings — elevated inflammatory cytokines, activated microglia, proliferating mast cells, damaged small fiber nerves, disrupted gut bacteria, and failing mitochondria. And there is a growing body of evidence suggesting that systemic nickel allergy syndrome (SNAS) may be part of the picture for a meaningful subset of patients.
This post walks through the research — what we know, what we do not know, and where the line falls between solid evidence and biological plausibility.
What Is Fibromyalgia?
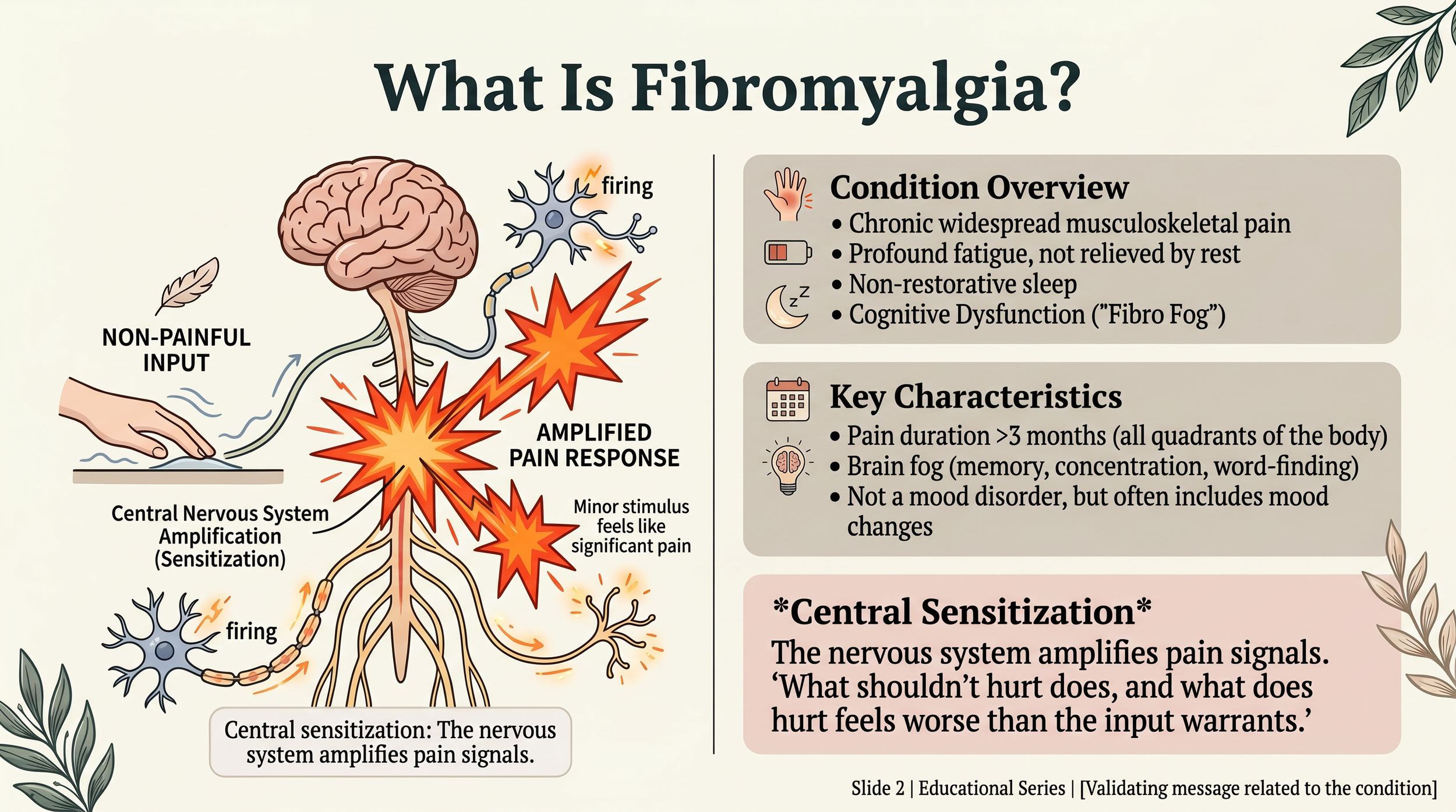
What is fibromyalgia?
Fibromyalgia is chronic widespread musculoskeletal pain lasting more than three months, accompanied by fatigue, cognitive dysfunction (“fibro fog”), and unrestorative sleep. It affects 2-4% of US adults — roughly 6 to 12 million people — and approximately 80% are women, with peak onset between ages 40 and 60.
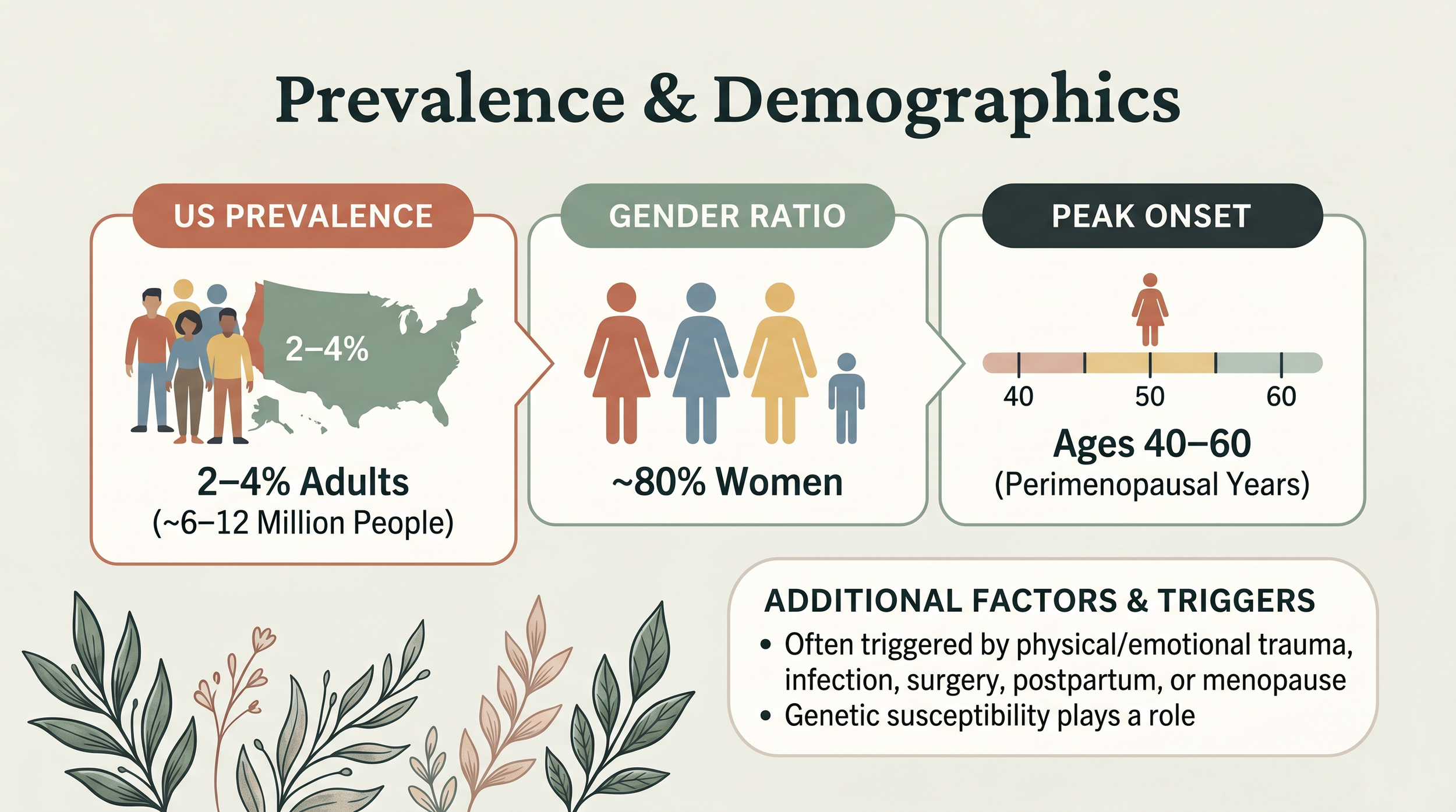
The prevalence and demographics of fibromyalgia
The hallmark feature is central sensitization: the nervous system amplifies pain signals so that stimuli that should not hurt do, and stimuli that should cause mild discomfort cause severe pain.
Diagnosis still relies on the 2016 American College of Rheumatology criteria — a combination of pain indices and symptom severity scores — and remains largely a diagnosis of exclusion. Most patients see four or more specialists over two to five years before receiving a diagnosis.
The Biology Is Real
When researchers look beyond clinical symptoms, they find consistent biological abnormalities in fibromyalgia patients:
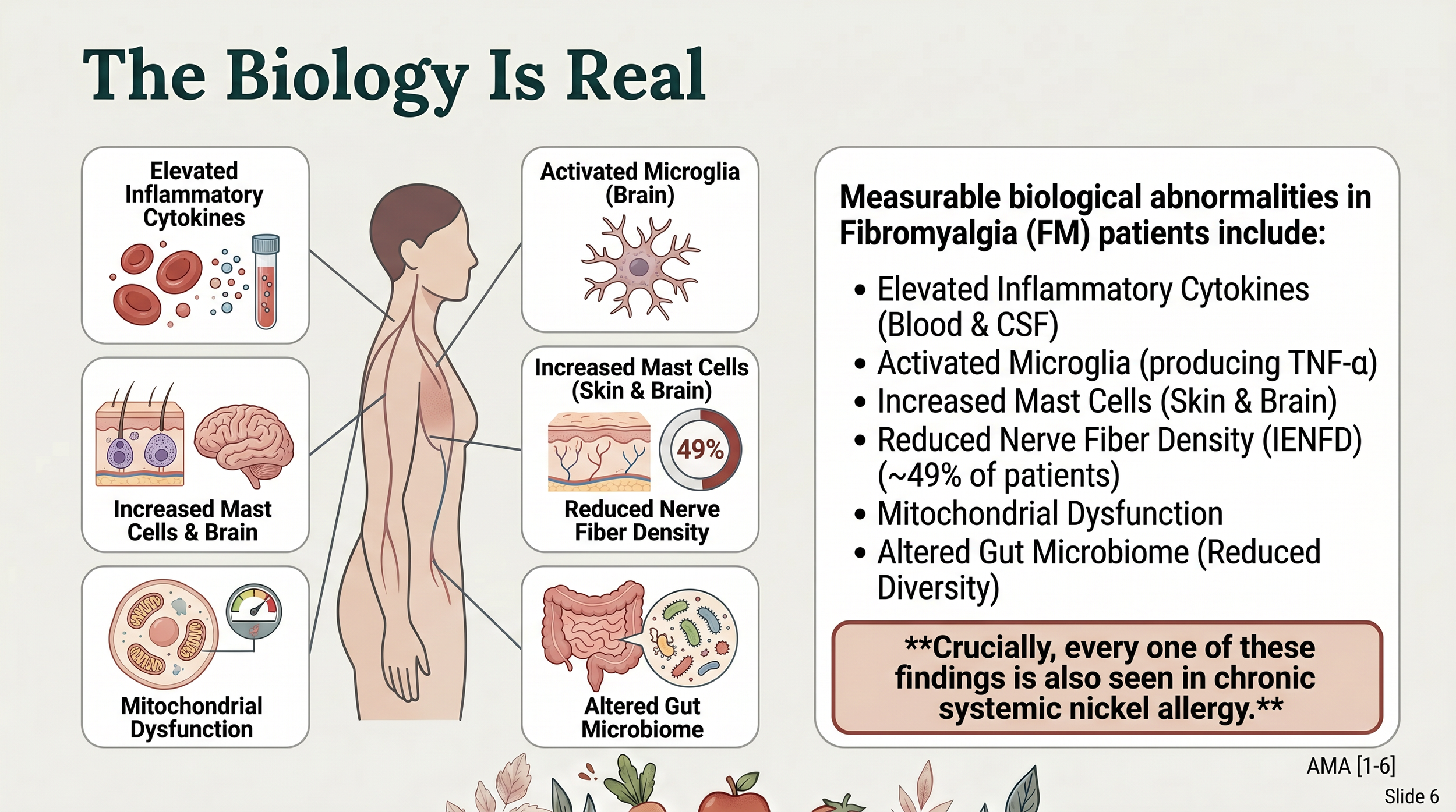
The biological mechanisms behind fibromyalgia. It’s not a fake disease.
Every one of these findings is also documented in chronic systemic nickel allergy as well!
How Common Is Nickel Allergy in Fibromyalgia?
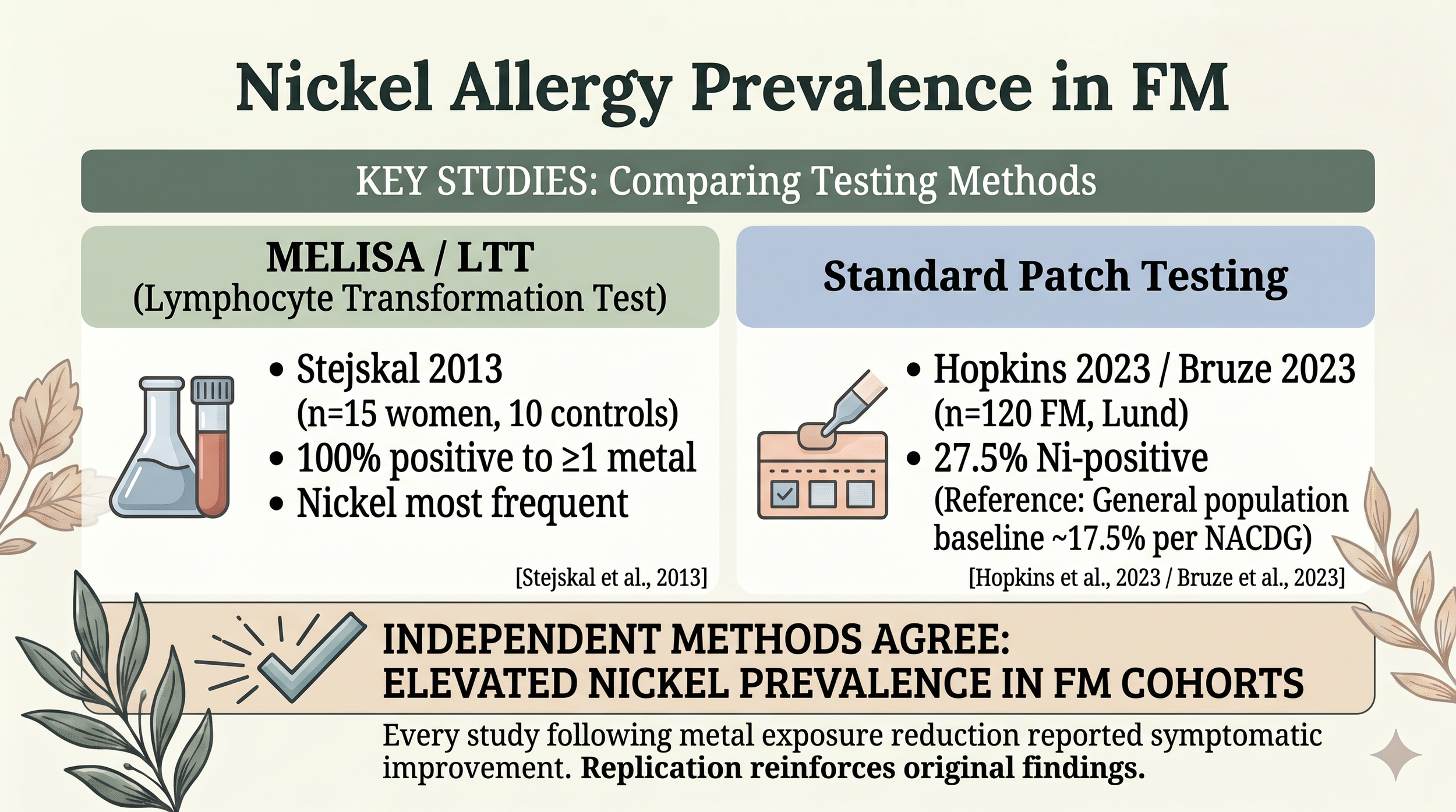
Multiple studies have examined nickel allergy prevalence in fibromyalgia patients. The general population baseline for nickel allergy by patch testing is approximately 17.5%.
The studies are small, but the original MELISA findings have been replicated by an independent dermatology group using standard patch testing. And every study that followed patients after reducing metal exposure found symptomatic improvement — including 50% of Stejskal’s cohort no longer meeting fibromyalgia diagnostic criteria after five years.
For more on testing methods, see our SNAS Testing deep dive.
Four Mechanisms That Connect Nickel to Fibromyalgia
Mechanism 1: Mast Cells
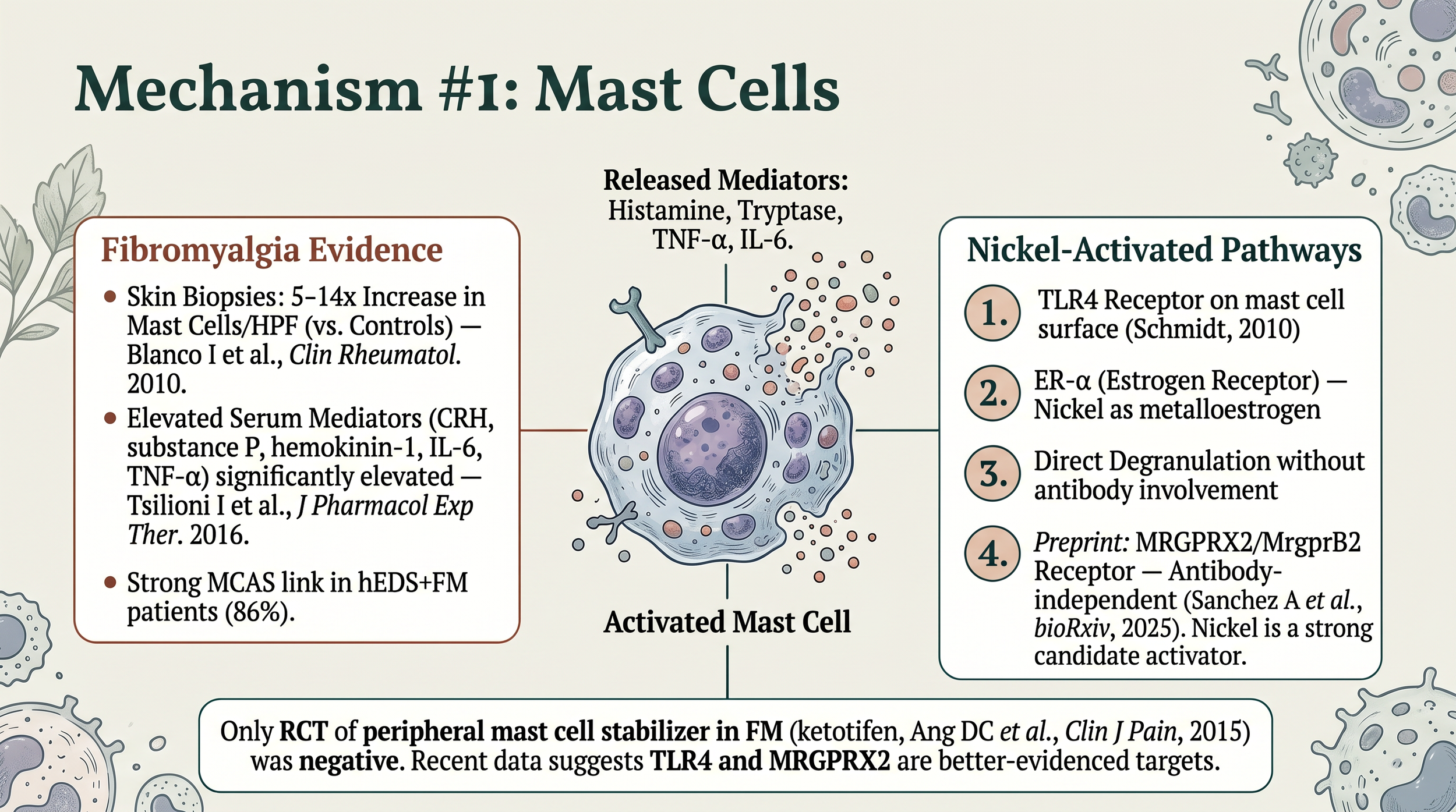
Mast cells are activated by nickel and impact fibromyalgia
Nickel activates mast cells through three simultaneous pathways — TLR4 receptor (Schmidt 2010), estrogen receptor alpha (metalloestrogen activity), and direct degranulation. A 2025 preprint adds a fourth potential pathway via MRGPRX2 (Sanchez A et al., bioRxiv. 2025 — not yet peer-reviewed).
Skin biopsies show 5-14x mast cell density in fibromyalgia versus controls (Blanco 2010), and serum mast cell mediators are significantly elevated (Tsilioni 2016). The one negative result: a ketotifen RCT in FM was negative (Ang 2015), but 2024-2025 data suggests it targeted the wrong pathway.
For a deeper look, see our MCAS and Mast Cells deep dive and our HIT and SNAS deep dive.
Mechanism 2: Cytokines and the Blood-Brain Barrier
The same inflammatory mediators that nickel produces in sensitized individuals — IL-1β, histamine, tryptase, TNF-α, VEGF — are the ones documented to damage the blood-brain barrier in fibromyalgia (Andrés-Rodríguez 2020; Ohgidani 2017). The “fibro fog” many patients experience may be inflammation crossing into brain tissue.
Our Brain Health deep dive covers this in detail.
Mechanism 3: Small Fiber Neuropathy
49% of fibromyalgia patients have measurable small fiber damage on skin biopsy (Grayston 2019). This is peripheral nerve loss — not a central nervous system imagination problem. Chronic mast cell activation produces tryptase, chymase, and TNF-α, all of which can damage small fibers. The same damage explains the 30-50% POTS (Postural Orthostatic Tachycardia Syndrome) overlap in fibromyalgia.
No study has directly tested whether nickel exposure correlates with small fiber loss in FM — this remains biological plausibility, not proven cause.
Mechanism 4: Gut Dysbiosis and SCFA Depletion
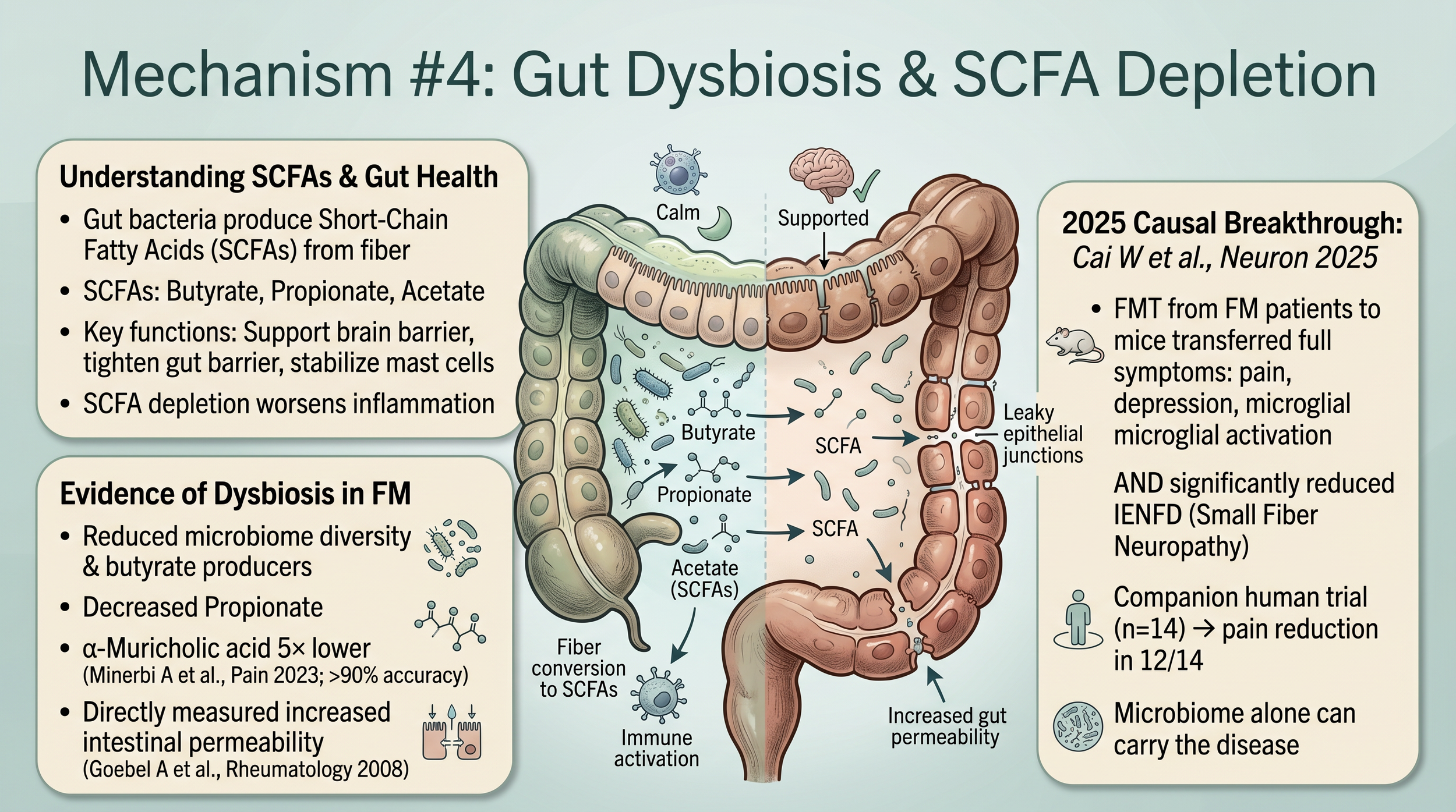
Fibromyalgia patients show reduced microbiome diversity, depleted propionate, and directly measured increased intestinal permeability (Goebel 2008). In 2025, Cai et al. published a landmark paper in Neuron (2025;113:2161-2175): fecal microbiota transplant from FM patients into germ-free mice transferred pain hypersensitivity, depression, microglial activation, altered metabolism, and reduced nerve fiber density. A companion human trial (n=14) showed pain reduction in 12 of 14 women.
The microbiome alone can carry the disease across species.
The well-formulated low-nickel diet with adequate fiber — resistant starch, PHGG, cooked-and-cooled potatoes — directly addresses this SCFA depletion. See our Fiber deep dive for practical guidance.
The Hormonal Angle: Why Perimenopause Matters
Fibromyalgia peaks during perimenopausal years (ages 40-60), earlier menopause correlates with worse outcomes (Martínez-Jauand 2013), and symptoms specifically worsen during menopause transition (Vidal-Neira 2024).
The mechanism: as natural estrogen falls, estrogen receptor alpha (ER-α) sites that were previously occupied become available. Nickel is a metalloestrogen — it can bind ER-α. But unlike estrogen, nickel on ER-α activates histamine pathways instead of providing protective pain modulation. Estrogen’s protective effects fade while nickel’s harmful effects amplify.
Mitochondria: The Convergence Point
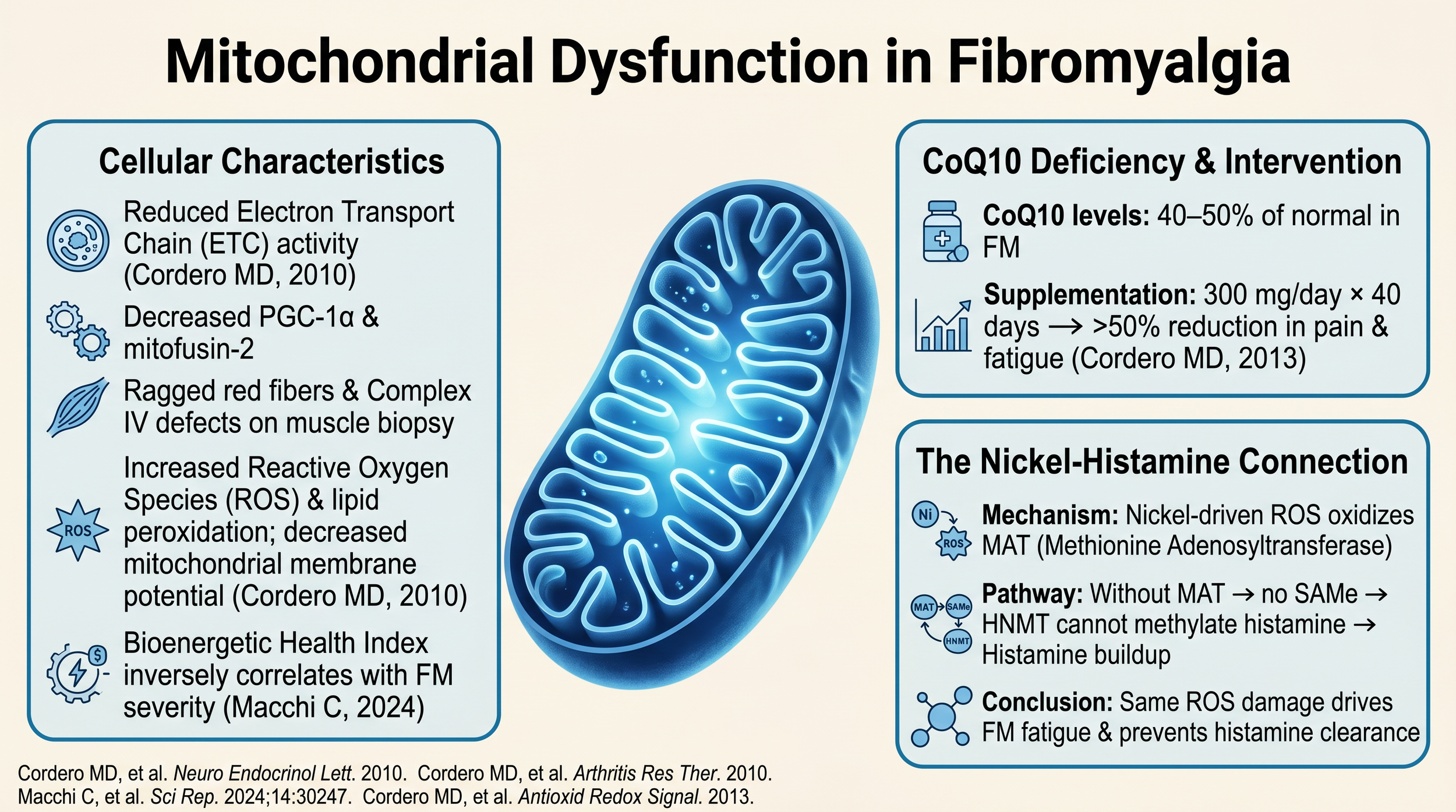
Supporting mitochondrial health is very important in fibromyalgia!
Fibromyalgia patients show reduced electron transport chain activity, ragged red fibers on muscle biopsy, increased reactive oxygen species, and CoQ10 levels at 40-50% of normal (Cordero 2010). The Bioenergetic Health Index inversely correlates with FM severity (Macchi 2024).
CoQ10 supplementation — 300 mg/day for 40 days — reduced pain and fatigue by more than 50% (Cordero 2013). CoQ10 is the electron shuttle in the mitochondrial assembly line; supplementing it directly supports repair of the bottleneck.
The nickel connection: nickel-driven reactive oxygen species oxidize MAT (methionine adenosyltransferase), blocking SAMe production, which prevents HNMT from methylating histamine. The same damage driving fatigue also prevents histamine clearance.
When sourcing CoQ10, choose synthetic, ICP-MS-tested products — “whole food” formulations often contain measurable nickel contamination. See our Deficiencies and Supplementation deep dive for brand guidance.
The Chelation Trap
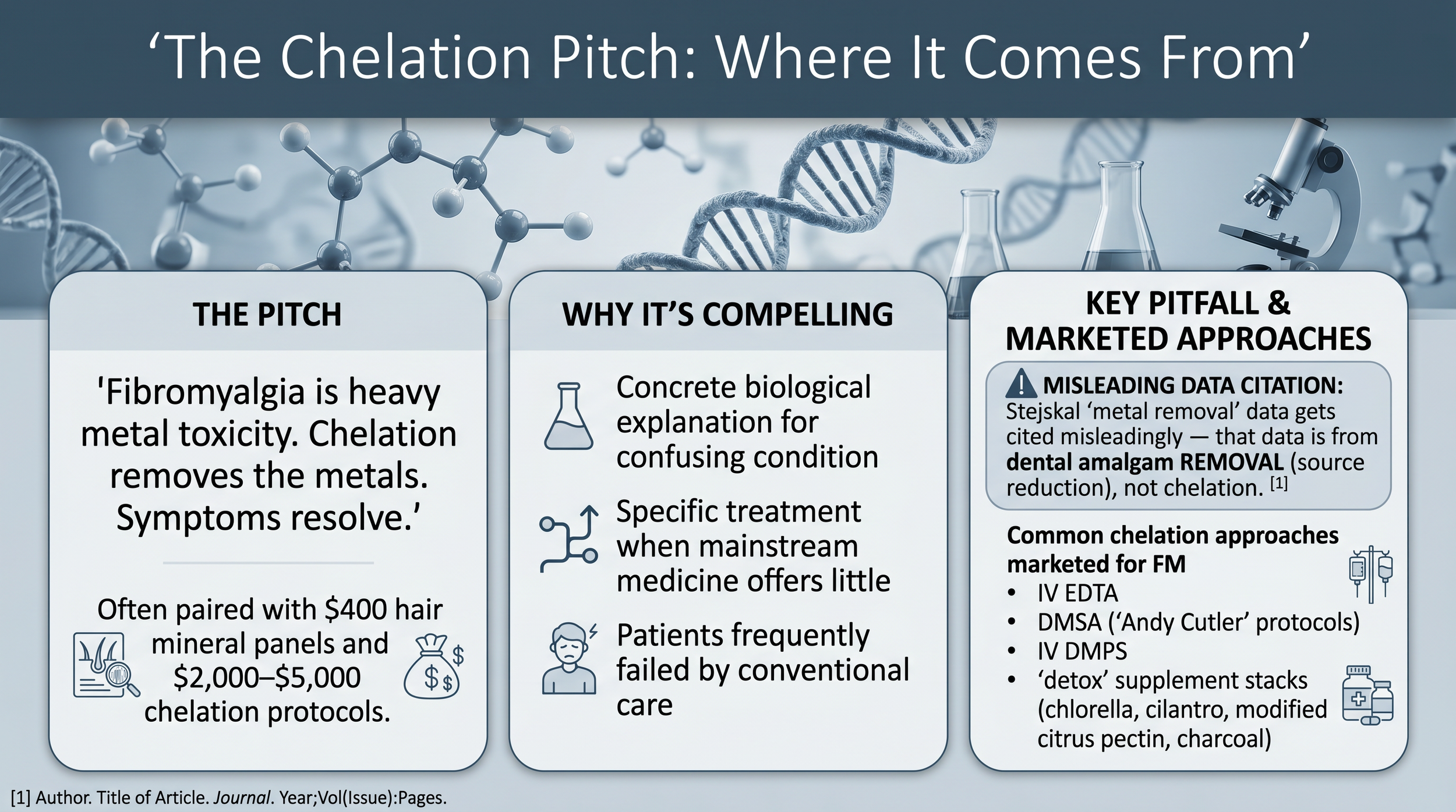
The reasons unethical naturopaths or health influencers give for chelation as a therapy for fibromyalgia.
If you have searched for metals and fibromyalgia online, you have likely seen chelation marketed as the solution. The pitch is compelling — it frames a confusing, dismissed condition as a concrete biological problem with a specific, actionable treatment.
The evidence base: zero RCTs with fibromyalgia as a primary outcome. Zero published case series. The Stejskal improvement data comes from dental amalgam removal (source reduction), not chelation — two completely different interventions.
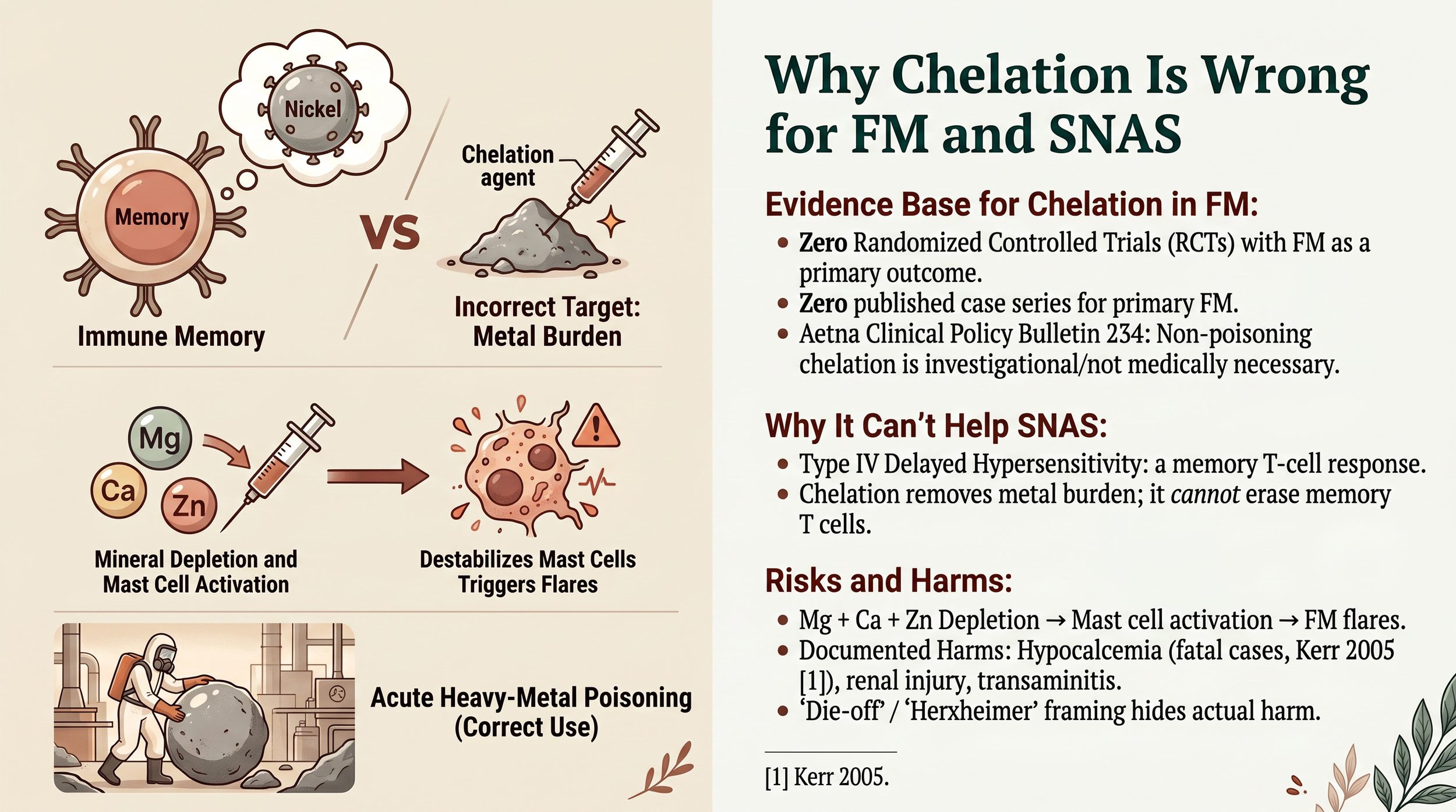
Why chelation cannot help fibromyalgia or systemic nickel allergy.
Why chelation cannot help SNAS: systemic nickel allergy is a Type IV delayed hypersensitivity — a memory T-cell response. The problem is immune memory, not metal burden. Chelation cannot erase memory T cells. And chelation agents deplete magnesium, calcium, and zinc — which destabilizes mast cells and can actively flare fibromyalgia and MCAS.
What works instead: reduce intake (the most powerful lever), adequate hydration, iron sufficiency (iron deficiency upregulates DMT1, increasing nickel absorption), sauna with mineral replacement, and sleep for glymphatic clearance. Nickel is freely filtered by the kidneys and does not bioaccumulate significantly. Once you stop overloading your body, your normal physiology handles what is already inside.
Diet Evidence in Fibromyalgia
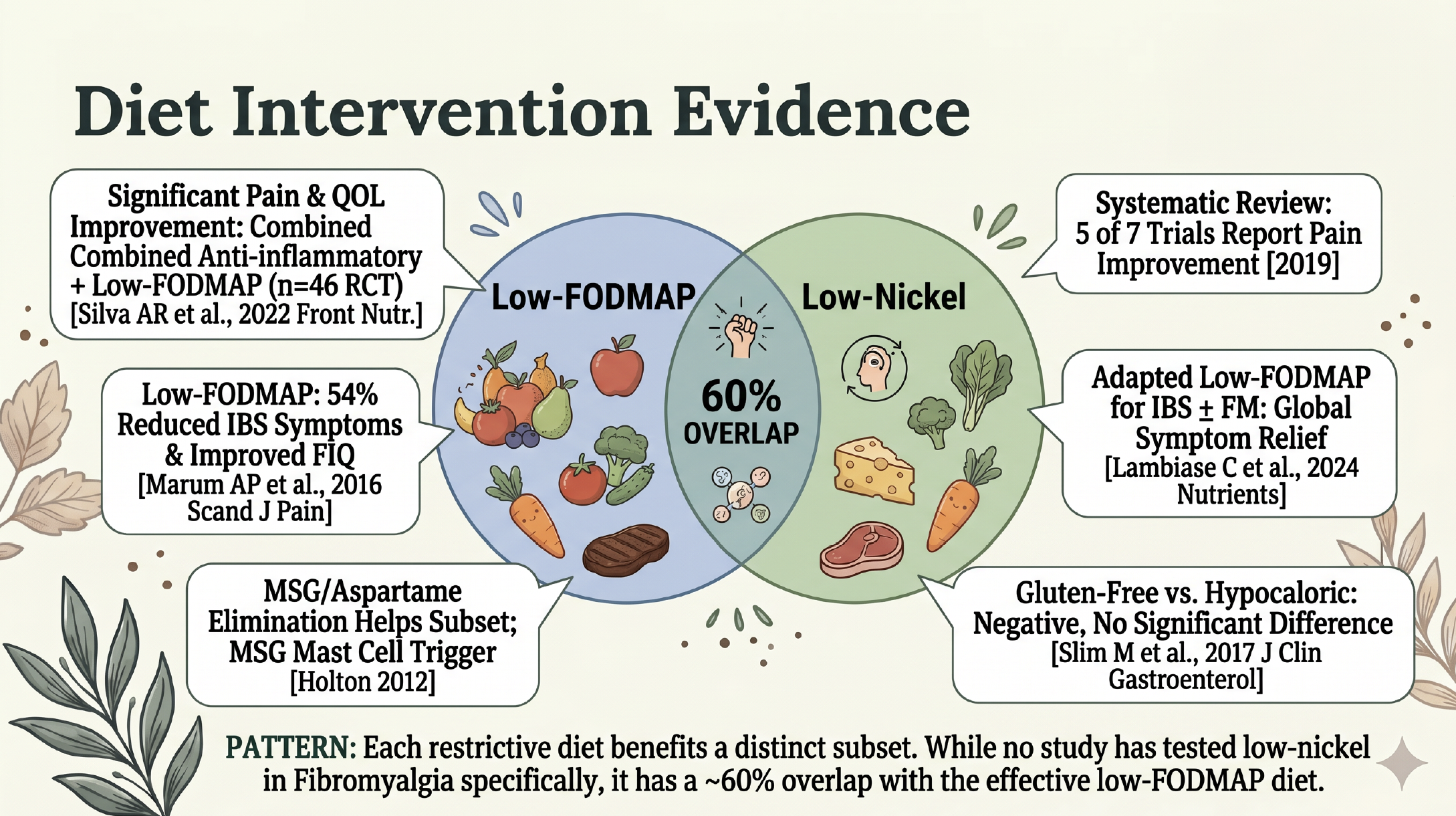
The pattern: every restrictive diet helps a subset. No study has tested low-nickel specifically in fibromyalgia. Low-FODMAP and low-nickel overlap approximately 60% — many “low-FODMAP responders” may be coincidentally lowering nickel intake.
The Supplement Landscape
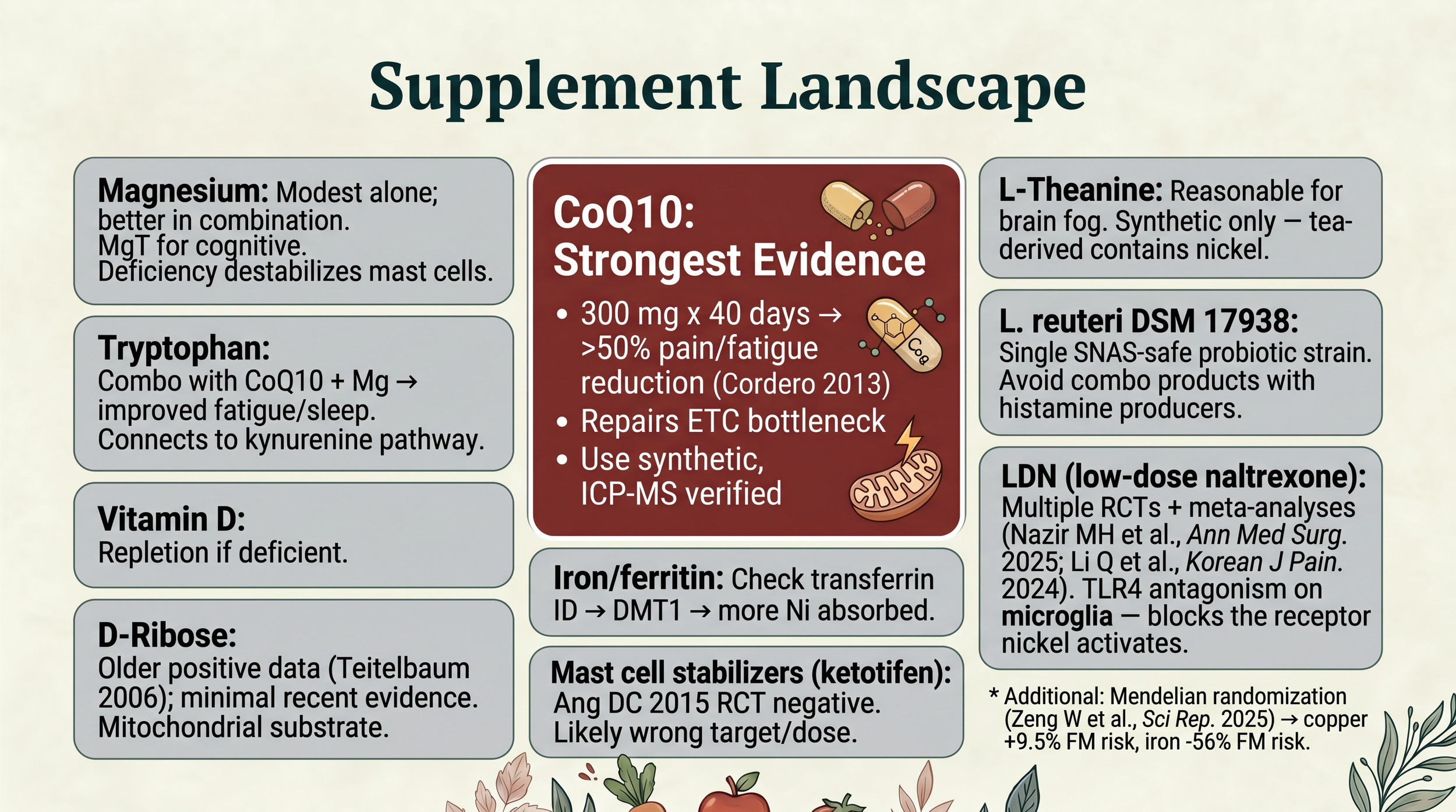
Supplements and their level of evidence for fibromyalgia and nickel allergy
Honest Limits of What We Know
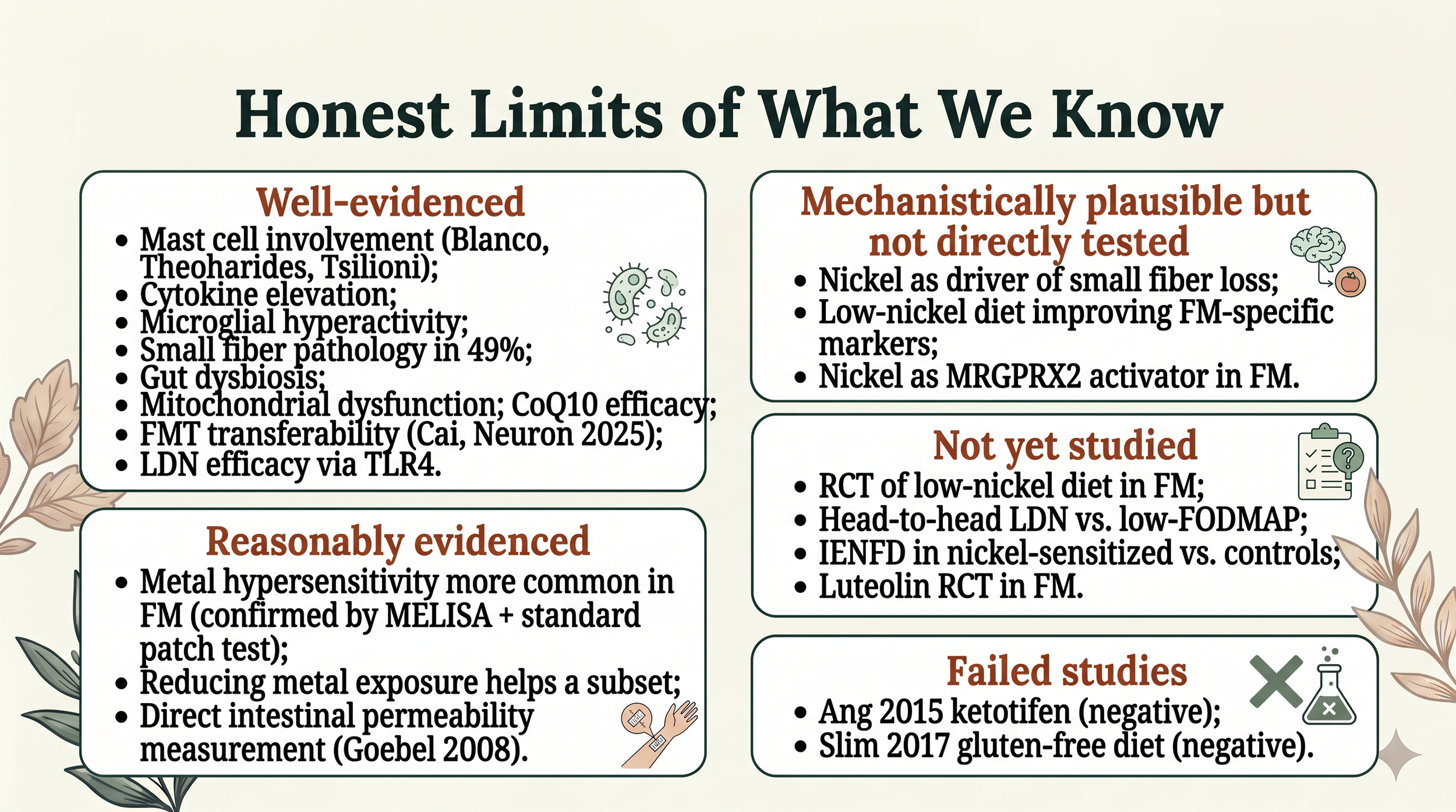
Well-evidenced: Mast cell involvement, cytokine elevation, microglial hyperactivity, small fiber pathology, gut dysbiosis, mitochondrial dysfunction, CoQ10 efficacy, FMT disease transfer (Cai 2025), LDN efficacy.
Reasonably evidenced: Metal hypersensitivity overrepresented in FM (two independent methods). Symptom improvement after metal exposure reduction. Intestinal permeability in FM.
Not yet tested: RCT of low-nickel diet in FM. Head-to-head low-nickel vs. low-FODMAP. Nickel-specific small fiber or mast cell quantification.
Negative studies: Ang 2015 ketotifen RCT. Slim 2017 gluten-free diet trial.
The convergence of evidence is strong enough to make exploring a low-nickel approach reasonable — especially since the intervention is safe and essentially free. But the definitive trial has not been run yet, and honesty about that matters.
What to Try: The Starter Plan
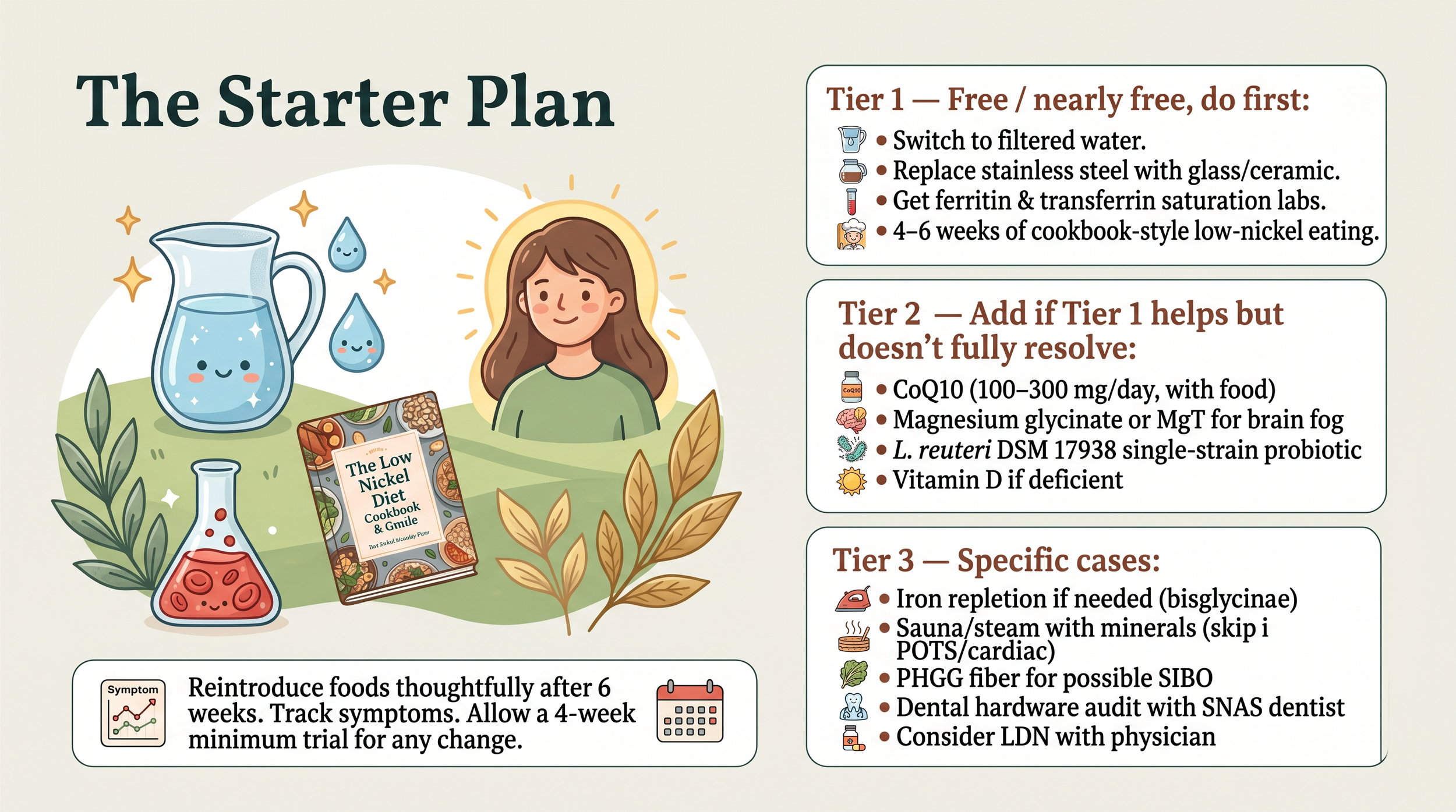
Tier 1 (free or nearly free):
Switch to filtered water; never drink first-draw water on an empty stomach
Replace stainless steel kettles, mugs, and travel bottles with glass or ceramic
Get ferritin AND transferrin saturation labs (request both)
Try 4-6 weeks of cookbook-style low-nickel eating
See our Water Filtration deep dive for filter guidance.
Tier 2 (if Tier 1 helps):
CoQ10 (100-300 mg/day, with food, low-Ni-tested)
Magnesium glycinate or magnesium threonate for brain fog
L. reuteri DSM 17938, single-strain probiotic
Vitamin D if deficient
Tier 3 (specific cases):
Iron repletion if labs indicate (alternate-day bisglycinate)
Sauna or steam 3-4x/week with mineral replacement (skip if POTS or cardiac concerns)
PHGG fiber if SIBO is on the table
Dental hardware audit with SNAS-aware dentist if multi-system symptoms persist
Consider LDN with your physician if pain is severe
Reintroduce thoughtfully after six weeks. Track your symptoms. Give any single change a four-week minimum trial before deciding if it is working.
Get the free Fibromyalgia & SNAS Starter Guide in my community or message me here on the site — It includes the decision framework, three-tier starter plan, key references for your doctor, and a supplement brand guide with the lowest-nickel options for CoQ10, magnesium, L-theanine, and more.
References
Andrés-Rodríguez L, Borrás X, Feliu-Soler A, et al. Immune-inflammatory pathways and clinical changes in fibromyalgia patients treated with mindfulness-based stress reduction (MBSR): a randomized, controlled clinical trial. Brain Behav Immun. 2020;80:109-119.
Ang DC, Hilligoss J, Stump T. Mast cell stabilizer (ketotifen) in fibromyalgia: a phase 1 randomized controlled clinical trial. Clin J Pain. 2015;31(9):836-842.
Blanco I, Beritze N, Argüelles M, et al. Abnormal overexpression of mastocytes in skin biopsies of fibromyalgia patients. Clin Rheumatol. 2010;29(12):1403-1412.
Cai W, et al. Fecal microbiota transplant transfers fibromyalgia phenotype. Neuron. 2025;113:2161-2175.e13.
Cordero MD, Alcocer-Gómez E, de Miguel M, et al. Can coenzyme Q10 improve clinical and molecular parameters in fibromyalgia? Antioxid Redox Signal. 2013;19(12):1356-1361.
Cordero MD, de Miguel M, Moreno Fernández AM, et al. Mitochondrial dysfunction and mitophagy activation in blood mononuclear cells of fibromyalgia patients. Arthritis Res Ther. 2010;12(1):R17.
Goebel A, Buhner S, Schedel R, et al. Altered intestinal permeability in patients with primary fibromyalgia and in patients with complex regional pain syndrome. Rheumatology (Oxford). 2008;47(8):1223-1227.
Grayston R, Czanner G, Elhadd K, et al. A systematic review and meta-analysis of the prevalence of small fiber pathology in fibromyalgia. Semin Arthritis Rheum. 2019;48(5):933-940.
Hopkins K, et al. Extended dental patch test series in fibromyalgia patients. Acta Derm Venereol. 2023.
Kim Y, et al. Short-chain fatty acids in fibromyalgia. Int J Environ Res Public Health. 2023.
Lambiase C, et al. Adapted low-FODMAP diet in IBS patients with fibromyalgia comorbidity. Nutrients. 2024;16(19):3419.
Li Q, et al. Low-dose naltrexone for fibromyalgia: a systematic review and meta-analysis. Korean J Pain. 2024.
Macchi C, Giachi A, Fichtner I, et al. Bioenergetic Health Index in fibromyalgia. Sci Rep. 2024;14:30247.
Martínez-Jauand M, et al. Early menopause and fibromyalgia. Clin Rheumatol. 2013.
Minerbi A, Gonzalez E, Brereton NJB, et al. Altered microbiome composition in individuals with fibromyalgia. Pain. 2019;160(11):2589-2602.
Minerbi A, et al. Serum bile acids in fibromyalgia. Pain. 2023.
Nazir MH, et al. Low-dose naltrexone in fibromyalgia: a systematic review and meta-analysis. Ann Med Surg (Lond). 2025.
Ohgidani M, Kato TA, Hosoi M, et al. Fibromyalgia and microglial TNF-α. Sci Rep. 2017;7:11882.
Palma-Ordóñez JF, et al. Gut microbiota in fibromyalgia: a systematic review. Int J Rheum Dis. 2024.
Pimentel M, et al. SIBO in fibromyalgia. Ann Rheum Dis. 2004.
Sanchez A, et al. MRGPRX2 / MrgprB2 in fibromyalgia IgG activation. bioRxiv. 2025 (preprint).
Silva AR, et al. Anti-inflammatory plus low-FODMAP diet in fibromyalgia (RCT). Front Nutr. 2022.
Slim M, et al. Gluten-free diet versus hypocaloric diet in fibromyalgia. J Clin Gastroenterol. 2017.
Tsilioni I, Russell IJ, Stewart JM, et al. Neuropeptides CRH, SP, HK-1 and inflammatory cytokines IL-6 and TNF are increased in serum of patients with fibromyalgia syndrome. J Pharmacol Exp Ther. 2016;356(3):664-672.
Vidal-Neira LF, et al. Fibromyalgia and menopause. Climacteric. 2024.
Zeng W, et al. Mendelian randomization of trace elements and fibromyalgia risk. Sci Rep. 2025.
This content is for educational purposes only and is not intended as medical advice, diagnosis, or treatment. The information presented is based on published, peer-reviewed research and is meant to help you have informed conversations with your healthcare provider. Always consult your doctor before making changes to your diet, supplements, or treatment plan. Individual results vary — what works for one person may not work for another.
Dr. Laura Duzett, DO NTP
The Low Nickel Diet
www.thelownickeldiet.com | Sundays 11 AM MST | Facebook & YouTube