Do I Have a Nickel Allergy? The Tests, the Myths, and What Actually Works
If you've been trying to figure out whether nickel is making you sick, you've probably run into a wall. Maybe your patch test came back negative and your dermatologist said you're fine. Maybe a naturopath ran a hair mineral analysis and told you your nickel is "high." Maybe a blood test came back borderline and nobody knew what to do next. Or maybe your GI doctor diagnosed IBS and never mentioned nickel at all.
Every one of those scenarios involves incomplete information — and it's not necessarily anyone's fault. Nickel allergy testing is genuinely confusing because nickel hypersensitivity isn't one condition. It shows up in three different locations in the body, each with different immune mechanisms, and most available tests only check for one.
After reviewing the peer-reviewed research, here's the uncomfortable truth: no single test can definitively diagnose dietary nickel allergy. But there is a clear path forward — and it doesn't require expensive labs or rare specialists.
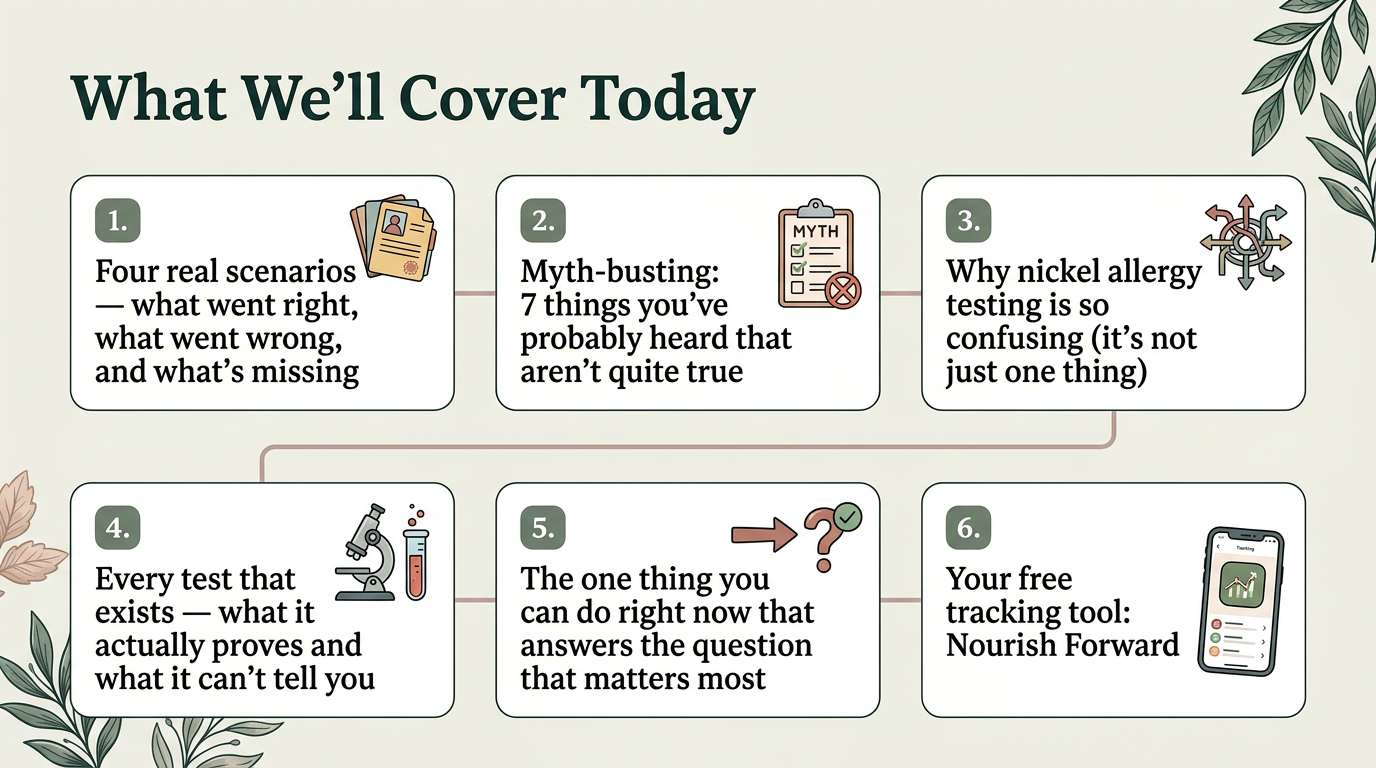
This article walks through every test that exists, the myths that waste your time and money, and the one thing you can do right now that answers the question that actually matters.
There Are Three Types of Nickel Allergy
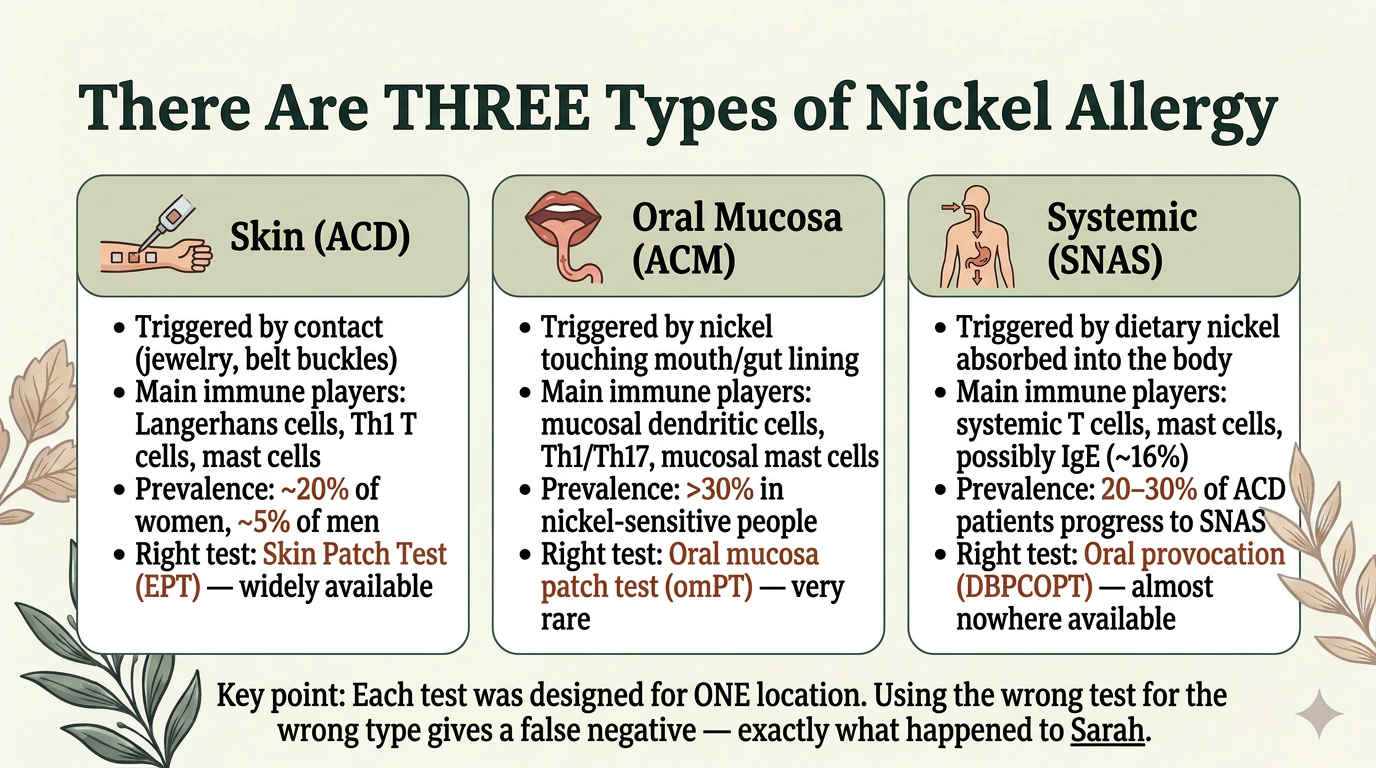
This is the framework that makes everything else make sense. Nickel hypersensitivity manifests in three distinct locations, each with different immune players and different diagnostic tools:
Skin (Allergic Contact Dermatitis / ACD) — triggered by direct contact with nickel-containing objects like jewelry, belt buckles, and phones. The immune response involves Langerhans cells and tissue-resident memory T cells in the skin. This is what the standard patch test detects. Prevalence: roughly 20% of women and 5% of men.
Oral Mucosa (Allergic Contact Mucositis / ACM) — triggered by nickel touching the lining of the mouth and gut. The mucosal immune system is fundamentally different from the skin — it uses different mast cells (mucosal mast cells vs. connective tissue mast cells), different T cell populations, and different immune signaling. Prevalence: potentially over 30% of nickel-sensitive people. Many are diagnosed with IBS instead.
Systemic (SNAS) — triggered by dietary nickel that's absorbed into the body and activates the immune system throughout. Involves both mast cell activation (direct, non-immunological degranulation — no IgE required) and delayed T-cell responses. An estimated 20-30% of people with skin nickel allergy eventually develop systemic reactions. Symptoms include GI distress, eczema flares at distant sites, headaches, brain fog, fatigue, and joint pain.
The critical point: Each test was designed for ONE location. The standard skin patch test checks the skin. It misses approximately 62% of people whose nickel allergy is systemic or mucosal. A negative patch test does not mean you don't have a nickel allergy — it means your skin didn't react.
The Myth-Busting: 7 Tests and Claims That Don't Do What You Think
"A negative patch test means you don't have a nickel allergy." — The patch test catches only about 38% of SNAS cases. Your gut can be reacting to dietary nickel even when your skin shows no response. The test answered correctly — it just answered the wrong question.
"A hair mineral analysis can show if you have too much nickel." — Studies show 10-fold differences between labs analyzing the same hair sample. Hair contains no immune markers. It can't distinguish between nickel inside your body and nickel from your shampoo or water. The AMA opposes this test for clinical use.
"IgG food panels identify nickel sensitivity." — IgG4 antibodies may actually indicate foods your body has learned to tolerate, not foods causing allergic reactions. Both the AAAAI and ACAAI recommend against using IgG panels for food allergy diagnosis.
"A blood test can diagnose nickel allergy." — The Lymphocyte Transformation Test (LTT) is real science. At optimized labs, it detects nickel sensitization with approximately 88% sensitivity and 96% specificity. But sensitization is not the same as clinical disease — many sensitized people never develop symptoms. The test also uses circulating blood cells, and the immune cells in your gut (tissue-resident memory T cells) don't circulate. It may miss gut-specific reactions entirely. And 92% of experts agree the test lacks standardization across labs.
"Serum nickel levels show if nickel is your problem." — Serum nickel measures exposure, not allergy. It was designed for occupational toxicity screening. You can be severely allergic with completely "normal" serum nickel levels.
"Bioresonance or electrodermal testing can detect nickel sensitivity." — No scientific validity. Rejected by the FDA and European health agencies.
"If your genetic test shows nickel-related variants, you're allergic." — FLG, TNF-alpha, and SLC30A3 variants increase risk, but predisposition does not equal active allergy. Many carriers never develop symptoms.
What Tests Actually Exist — and What Each One Can (and Can't) Tell You
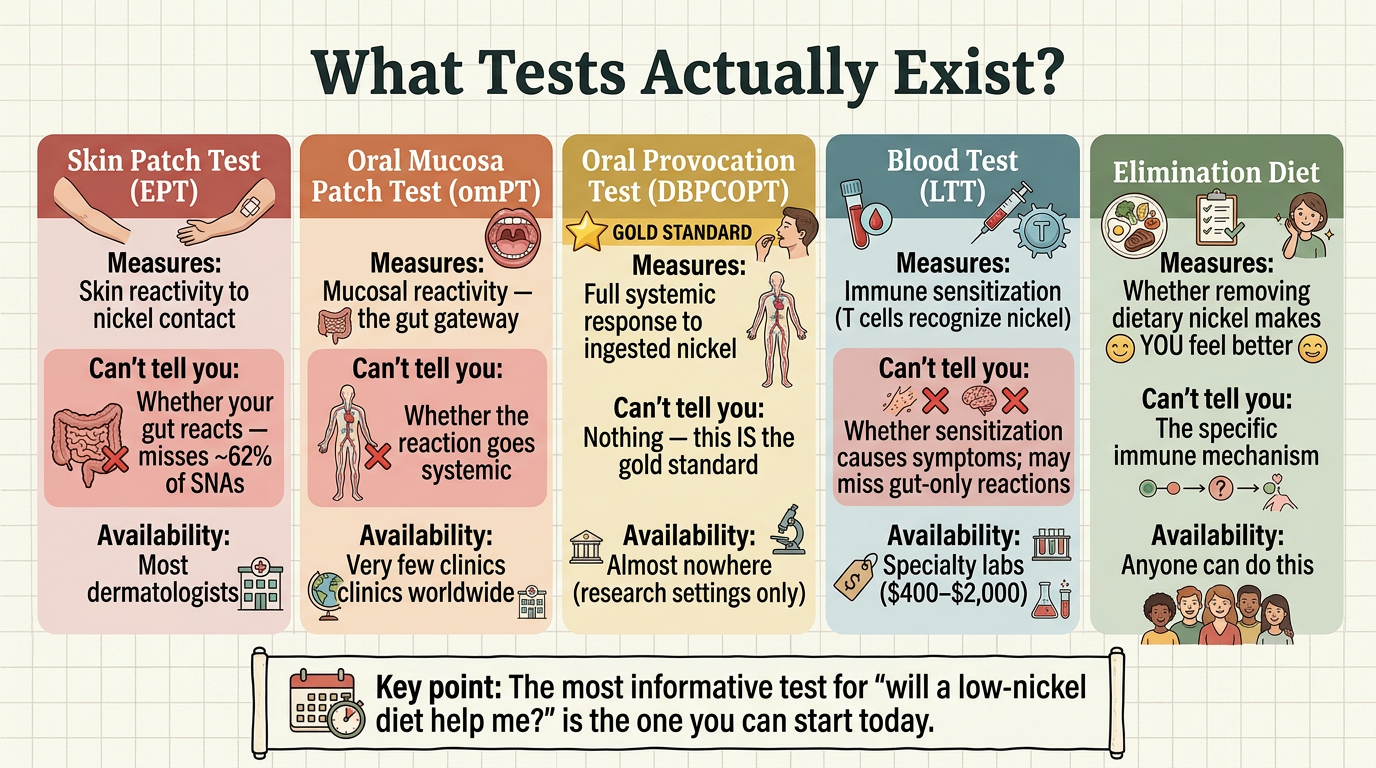
Skin Patch Test (EPT): Tests: Skin reactivity to nickel contact and whether your gut reacts — It misses ~62% of SNAS
Oral Mucosa Patch Test (omPT): Tests: Mucosal reactivity — the gut gateway, It doesn’t test whether the reaction goes systemic, and it is available in very few clinics worldwide (mostly research)
Oral Provocation (DBPCOPT): Tests: Full systemic response to ingested nickel — the gold standard. This IS the definitive test but it’s available almost nowhere (research settings only)
Blood Test (LTT/NiLPT) Tests: Immune sensitization (T cells recognize nickel), but doesn’t test whether sensitization causes symptoms; and it may miss gut-only reactions. Available in Specialty labs ($400–$2,000)
Elimination Diet: Tests: Whether removing dietary nickel makes YOU feel better, doesn’t test the specific immune mechanism. ANYONE CAN DO THIS and this is how I was diagnosed by my dermatologist.
The most informative test for the question that actually matters — "will a low-nickel diet help me?" — is the one you can start today.
Sensitization vs. Clinical Disease: The Distinction That Changes Everything
Sensitization means your immune system recognizes nickel. This is what blood tests measure. Clinical disease means nickel is actively making you sick. This is what provocation tests and elimination diets measure.
You can be sensitized and never get symptoms. You can also have symptoms driven by nickel through non-immune pathways — normal gut absorption, direct mast cell degranulation, barrier permeability — even if a blood test says you're not classically sensitized. The overwhelming majority of SNAS patients (~84%) do NOT have nickel-specific IgE. Their mast cell symptoms come from direct degranulation and T-cell-mediated activation — not from Type I hypersensitivity. This is why standard allergy testing that looks for IgE misses SNAS entirely.
This is also why the elimination diet is so powerful. It bypasses the mechanistic question and asks the one that matters: "Does this help YOU?"
The MCAS, Histamine Intolerance, and IBS Connection
If you have Mast Cell Activation Syndrome, histamine intolerance, or an IBS diagnosis, nickel may be one of the triggers your body is reacting to — even if it's not the only one.
Nickel activates TLR4 (the same receptor that responds to bacterial toxins), triggering inflammation without classical allergy. It directly degranulates mast cells without requiring IgE. It disrupts tight junctions through the tryptase/PAR-2 pathway, increasing gut permeability. And VEGF released by activated mast cells drives the vascular remodeling that sustains chronic inflammation and establishes the gut-skin axis — which is how eating nickel-rich food can cause skin flares at distant sites.
An estimated 30% or more of IBS patients may have unrecognized nickel allergy. The low-FODMAP diet partially helps some of these patients because it coincidentally removes some high-nickel foods — but it doesn't address the root cause.
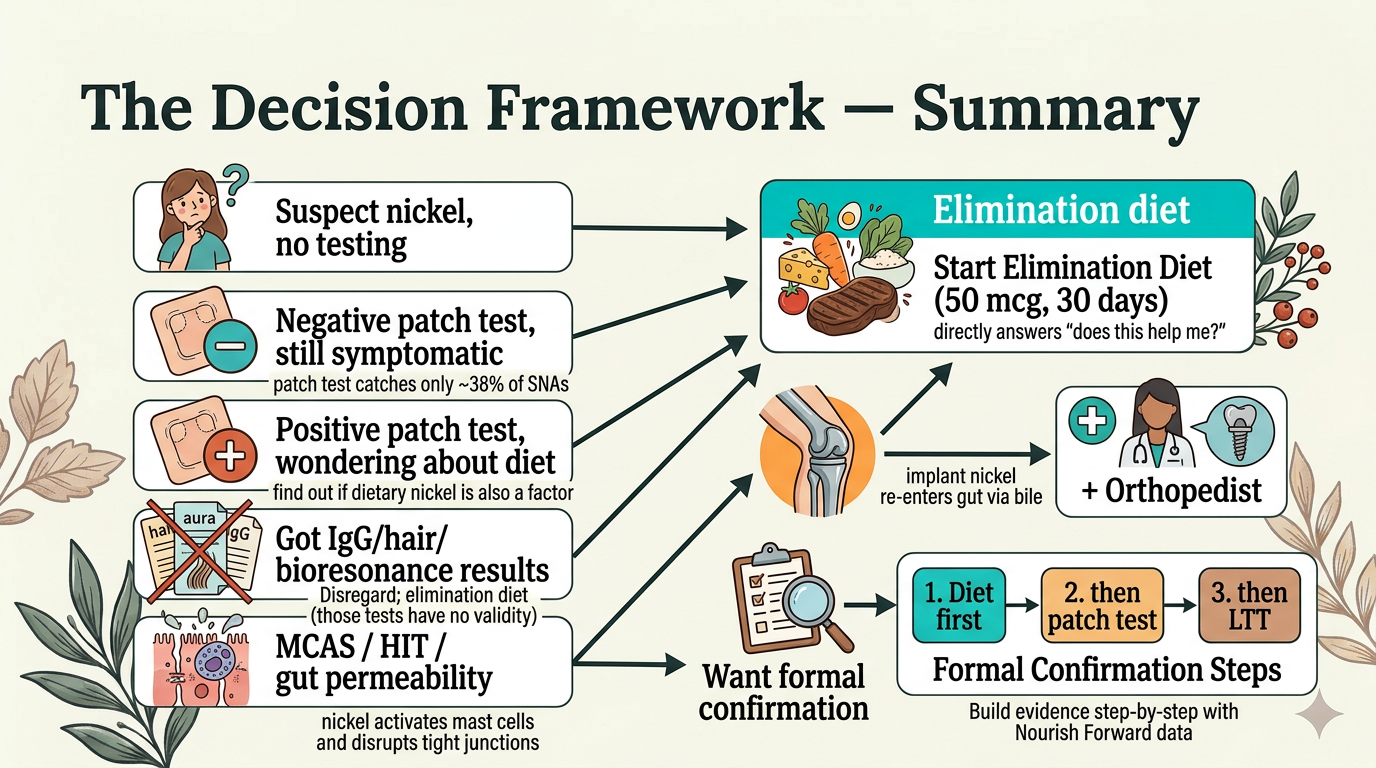
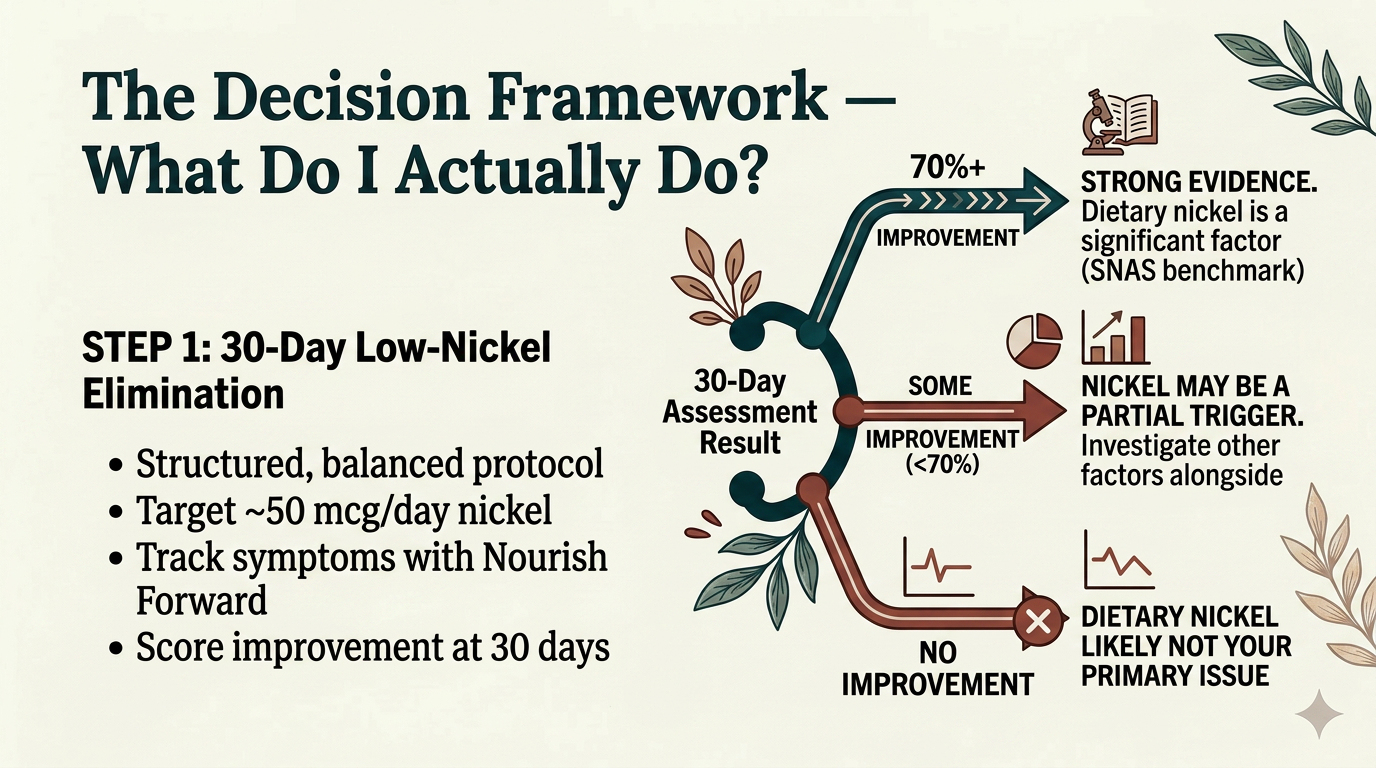
The Decision Framework: What Should You Actually Do?
Why 50 mcg? The Science Behind the Starting Point
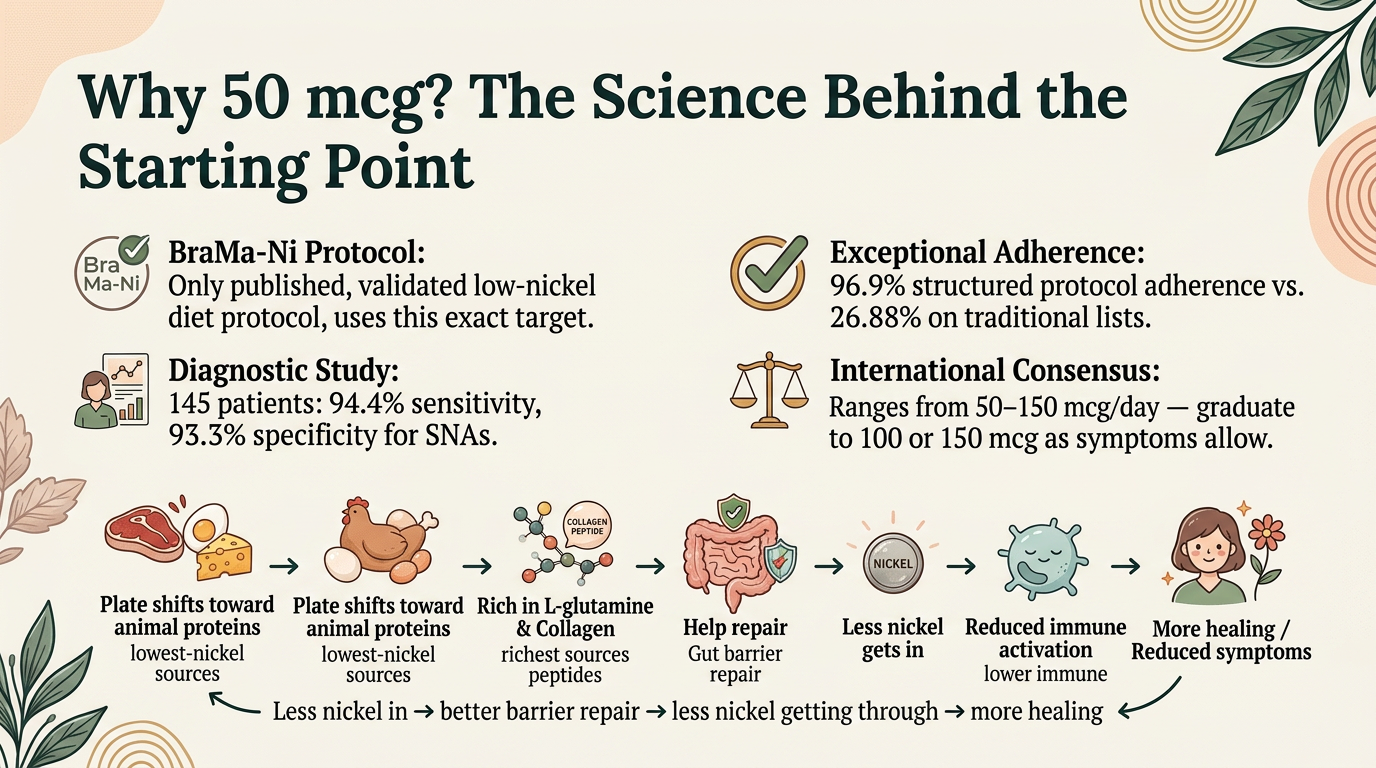
The BraMa-Ni protocol is the only published, validated low-nickel diet protocol. It targets approximately 50 mcg of nickel per day, and in a study of 145 patients it achieved 94.4% sensitivity and 93.3% specificity for identifying SNAS. Adherence on the structured protocol was 96.9%, compared to just 26.8% on traditional "forbidden food" lists.
International consensus ranges from 50–150 mcg/day. Starting at 50 mcg naturally shifts your plate toward animal proteins — the lowest-nickel whole food sources and the richest sources of L-glutamine and collagen peptides that help repair the gut lining. This creates a virtuous cycle: less nickel in, better barrier repair, less nickel getting through, reduced immune activation, more healing.
After 30 days, score your improvement: 70% or better is the benchmark researchers use to confirm SNAS. Some improvement but less than 70% suggests nickel is part of the picture alongside other triggers. No improvement suggests dietary nickel probably isn't your primary issue.
If the Diet Helps — What Comes Next?
Step 2: Talk to your dermatologist about a patch test (EPT). Most widely available. A positive result confirms contact sensitization. A negative result still doesn't rule out SNAS — but it's a start.
Step 3: Oral mucosa patch test (omPT). Catches roughly 62% of SNAS vs. 38% for the skin patch. Very few clinics worldwide currently offer this.
Step 4: Blood test (LTT/NiLPT). Available at National Jewish Health in Denver, IMD Berlin, and MELISA labs internationally. Costs $400–$2,000 and is rarely covered by insurance.
Step 5: Oral provocation test (DBPCOPT). The gold standard — three placebos and five active doses over eight days. Currently available almost exclusively in research settings.
What's Coming: The Future of Testing
Research has identified IL-5 (not IFN-gamma) as the strongest biomarker for nickel allergy severity. Nickel-specific IL-5 secretion correlates significantly with the intensity of positive patch test reactions, while IFN-gamma does not. Cytokine-profiling blood tests that measure IL-5 alongside proliferation could transform diagnosis — but they aren't widely available yet.
The NILT clinical trial (NCT07105865) is currently studying nickel and lipid transfer proteins in functional GI disorders. AI-powered proteomic biomarkers are being explored to predict treatment response. And combination panel testing — cytokine profile plus provocation plus dietary response — is likely the future of SNAS diagnosis.
For now, the elimination diet remains the most accessible and most informative tool available.
The Bottom Line
There are three types of nickel allergy, and most tests only check for one. A negative patch test does not rule out dietary nickel allergy. Hair mineral analysis, IgG panels, serum nickel, bioresonance, and genetic tests are not valid for nickel allergy diagnosis. The blood test (LTT) is real science but measures sensitization, not disease. The gold standard oral provocation test exists almost nowhere.
But the structured elimination diet — using the same 70% improvement benchmark that researchers use — answers the question that matters most. And you can start it today.
Track your symptoms with Nourish Forward (free and YOU own your data - I have no access to it), bring your data to your doctor, and build the evidence step by step.
This article is for educational purposes only and is not intended as medical advice, diagnosis, or treatment. The information presented is based on published, peer-reviewed research and is meant to help you have informed conversations with your healthcare provider. Always consult your doctor before making changes to your diet, supplements, or treatment plan. Individual results vary — what works for one person may not work for another.
References
Braga M et al. Systemic Nickel Allergy Syndrome: nosologic framework and usefulness of diet regimen for diagnosis. Int J Immunopathol Pharmacol. 2013;26(3):707-716.
Jensen CS, Menné T, Johansen JD. Systemic contact dermatitis after oral exposure to nickel: a review with a modified meta-analysis. Contact Dermatitis. 2003;68(1):3-14.
Ricciardi L et al. Oral nickel challenge and systemic symptoms. Int J Immunopathol Pharmacol. 2014;27(1):131-135.
Borghini R et al. Oral mucosa patch test in systemic nickel allergy syndrome. Contact Dermatitis. 2020;83(5):391-397.
Muris J et al. Poor correlation among metal hypersensitivity testing modalities. Contact Dermatitis. 2022;88(1):26-33.
Schalock PC et al. Expert consensus on metal implant allergy diagnostics. J Dtsch Dermatol Ges. 2024.
Schmidt M et al. Crucial role for human TLR4 in the development of contact allergy to nickel. Nat Immunol. 2010;11:814-819.
Kinbara T et al. Mast cell histamine-mediated transient inflammation following exposure to nickel promotes nickel allergy. Exp Dermatol. 2016;25(6):466-471.
Santucci B et al. Immunological characterization of the allergic contact mucositis related to the ingestion of nickel-rich foods. Contact Dermatitis. 2014;71(6):364-370.
Picarelli A et al. Oral mucosa patch test: a new tool to recognize and study the adverse effects of dietary nickel exposure. Biol Trace Elem Res. 2011;139(2):151-159.
Vital M et al. Revealing the bacterial butyrate synthesis pathways. mBio. 2014;5(2):e00889-14.
Systemic Nickel Allergy Syndrome overview. PMC 4406458.
Telenutrition for SNAS management. MDPI Nutrients. 2021.
Expert consensus on LTT standardization. PMID: 28176340.