Dyshidrotic Eczema and Systemic Nickel Allergy: Why Your Hands or Feet Won't Heal
Dyshidrotic Eczema and Systemic Nickel Allergy: Why Your Hands or feet Won't Heal
If you're dealing with painful, itchy blisters on your hands or feet that keep coming back no matter what cream your dermatologist prescribes — your food might be the cause.
80% of patients with chronic nickel-related dermatitis achieved complete or near-complete recovery on a low nickel diet (Antico & Soana, 2015). And most of them had been stuck in a cycle of steroid creams for years before anyone connected their skin to their plate.
What Is Dyshidrotic Eczema?
Dyshidrotic Hand & Foot eczema or pompholyx is a deeply itchy blistery mess of a condition!
Dyshidrotic eczema — also called pompholyx — is characterized by deep, intensely itchy blisters on the palms of the hands and soles of the feet. It's usually treated as a standalone skin problem with topical steroids, which suppress symptoms temporarily but never resolve the underlying cause.
In many patients, dyshidrotic eczema is actually a manifestation of Systemic Contact Dermatitis — meaning the trigger isn't something touching your skin. It's something you're eating.
How Food Causes Blisters on Your Hands
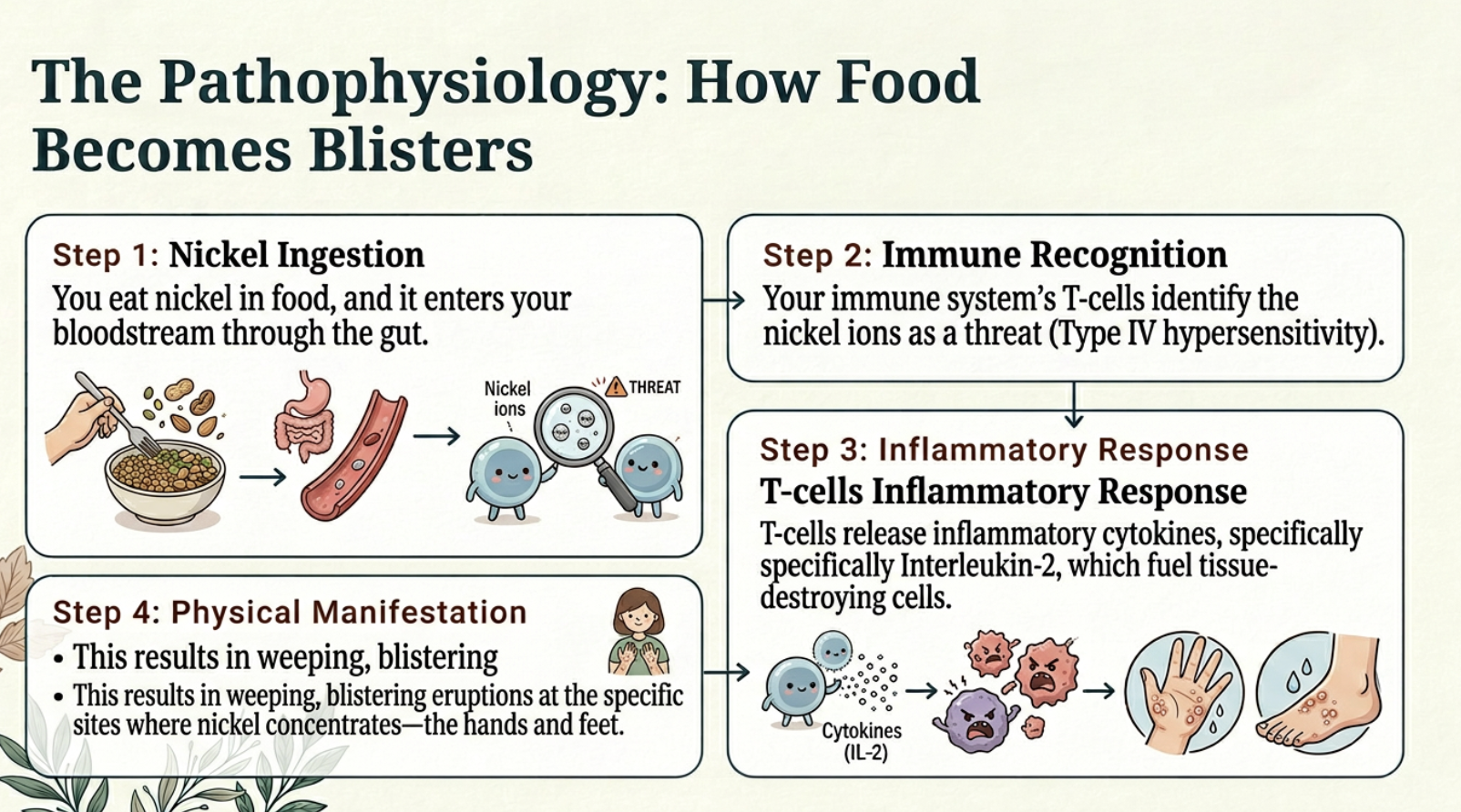
Here's the pathway: you eat nickel in food → it enters your bloodstream → your immune system's T-cells identify nickel as a threat → T-cells release inflammatory cytokines (like Interleukin-2) that fuel tissue-destroying cells → result: weeping, blistering eruptions.
But why specifically on the hands and feet? This is where the science gets fascinating.
The Sweat Connection
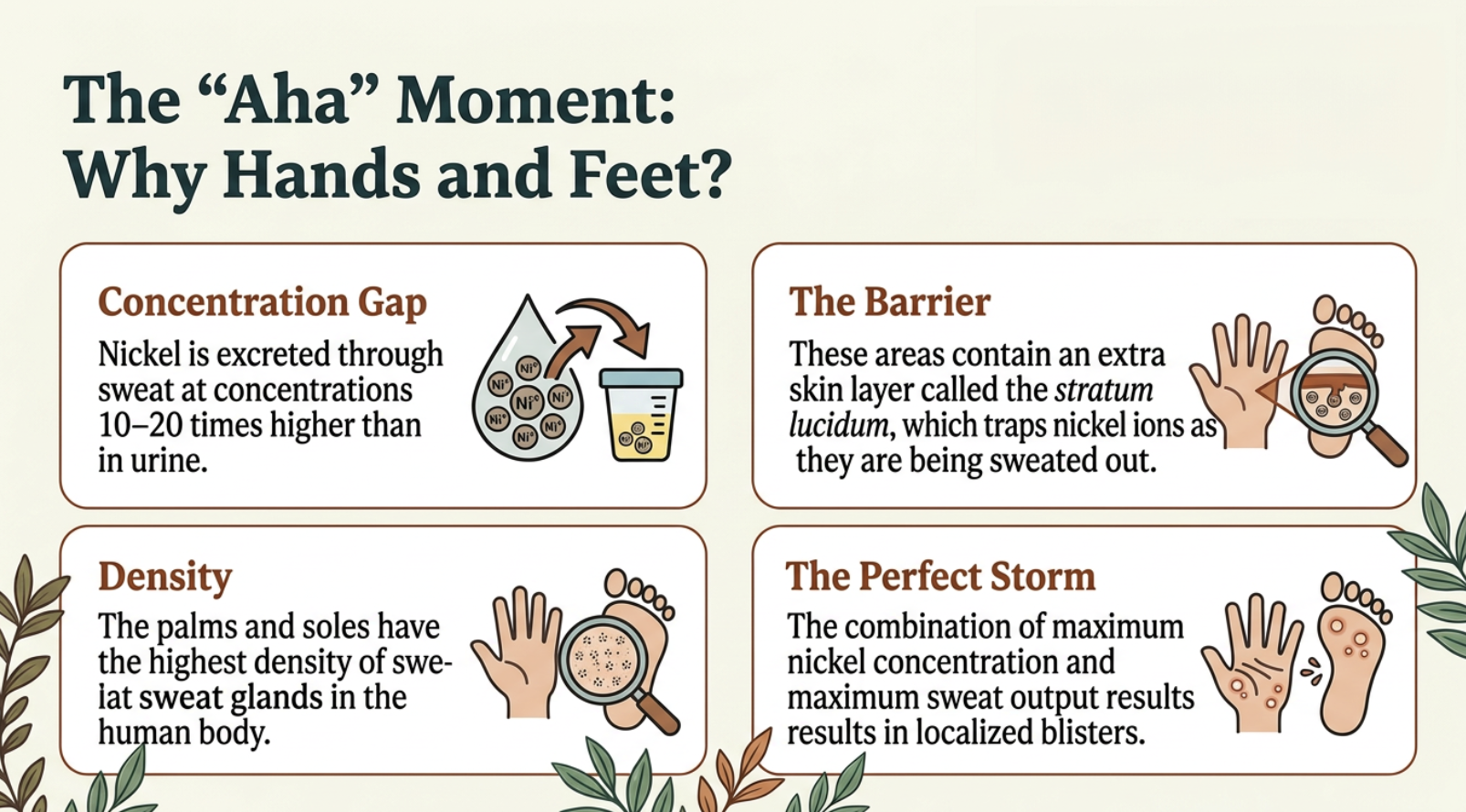
Nickel absorbed from food is excreted through feces, urine, and sweat. But here's the critical detail: nickel concentrations in sweat are 10 to 20 times higher than in urine.
And where does your body have the highest density of sweat glands? Your palms and soles.
These areas also have an extra layer of skin called the stratum lucidum, which traps nickel ions as they're sweated out. Maximum nickel concentration plus maximum sweat output plus a skin layer that traps the metal — it creates a "perfect storm" for localized allergic blistering.
Your body is trying to get rid of the nickel through your sweat. But your palms and soles have the most sweat glands AND an extra layer that traps the nickel as it comes out. It's like a traffic jam of nickel ions right under the surface of your hands.
The Clinical Proof
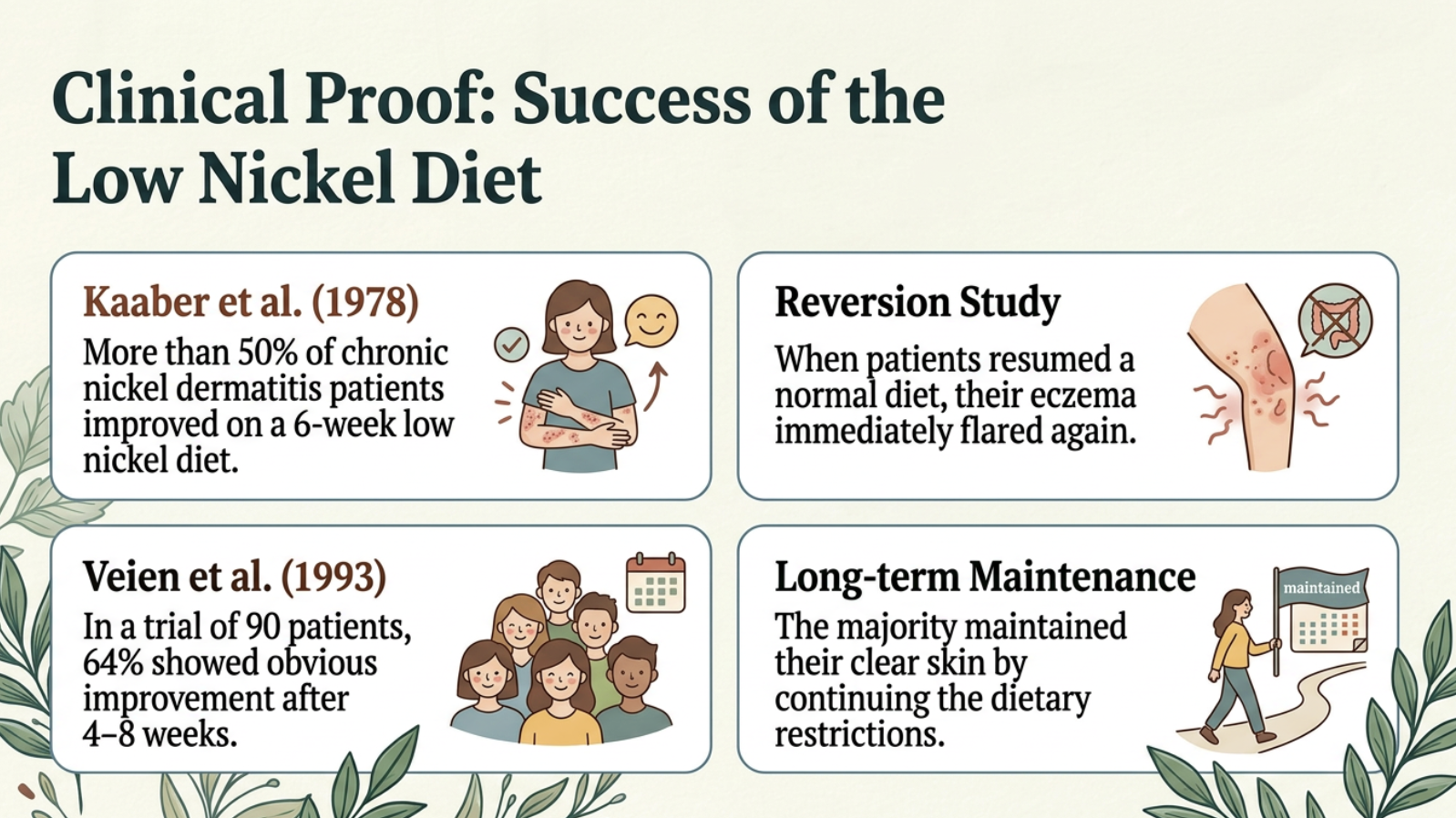
In a foundational study, over 50% of patients with chronic nickel dermatitis improved on a 6-week low nickel diet. When 7 of those patients resumed a normal diet, their hand eczema immediately flared (Kaaber et al., 1978).
In a larger 90-patient trial, 64% showed obvious improvement after 4 to 8 weeks on a low nickel diet, and the majority maintained that improvement long-term by continuing the diet (Veien et al., 1993).
And in oral challenge studies, where patients who had cleared on a low nickel diet were given a blinded nickel capsule, 89% experienced an acute flare-up of their skin symptoms (Picarelli et al., 2010). They were clear. They took one pill. 89% flared. The food-to-skin connection is proven.
In another classic study specifically examining hand eczema, 75% of patients flared immediately when given a nickel pill (Veien & Kaaber, 1979).
Why Steroid Cream Isn't Enough
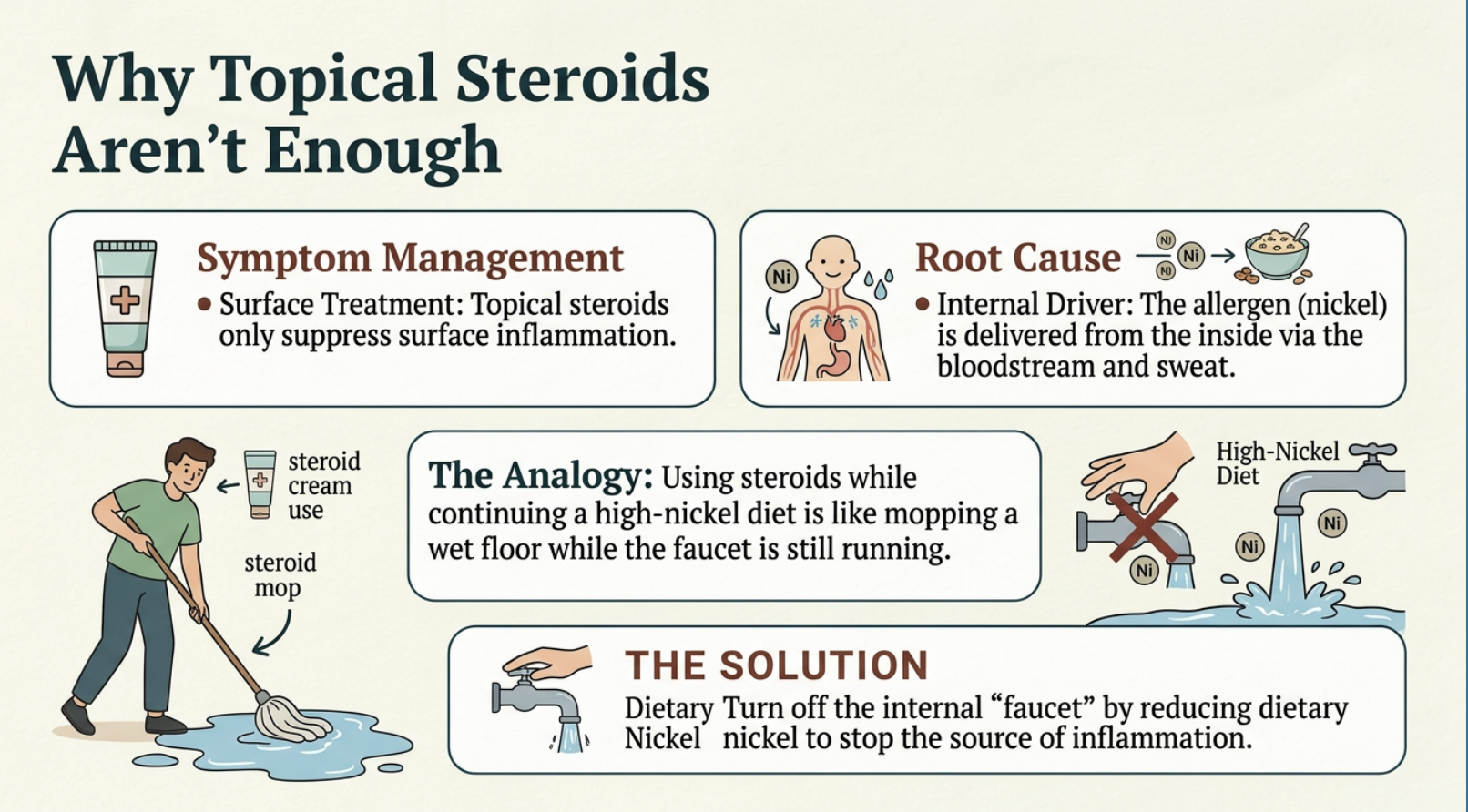
Steroid cream isn’t enough for dyshidrotic hand and foot eczema caused by nickel
Topical steroids suppress surface inflammation. But if the allergen is being delivered from inside your body via your bloodstream and sweat, the internal "faucet" is still running.
Imagine trying to mop a wet floor while the faucet is still on. That's what steroid cream does when dietary nickel is the driver. You have to turn off the faucet first — and the faucet is your diet.
The Negative Patch Test Trap
Here's a misconception that keeps people stuck for years: some patients with classic dyshidrotic eczema test negative on the standard skin patch test but still flare on oral nickel challenge. In those cases, the allergy is driven by mucosal or systemic absorption, and may require an Oral Mucosa Patch Test or a dietary elimination trial to properly diagnose.
A negative patch test does NOT rule out nickel as your trigger.
Your Next Step
If you have dyshidrotic eczema and this sounds like your story, the most immediate, actionable step is to find out which foods in your diet are high in nickel. Download my free Nickel Food List to start identifying your triggers.
Download the Free Nickel Food List →
Next in the series: which supplements are safe for SNAS patients — and which ones might be making you worse.
References
Antico A, Soana R. Nickel sensitization and dietary nickel are a substantial cause of symptoms provocation in patients with chronic allergic-like dermatitis syndromes. Allergy Rhinol (Providence). 2015;6(1):e56-e63.
Bergman D, Goldenberg A, Rundle C, Jacob SE. Low Nickel Diet: A Patient-Centered Review. J Clin Exp Dermatol Res. 2016;7(3):355.
Calogiuri GF, Bonamonte D, Foti C, Al-Sowaidi S. Nickel Hypersensitivity: A General Review on Clinical Aspects and Potential Co-Morbidities. J Allergy Ther. 2016;7(5):243.
Christensen OB, Möller H. External and internal exposure to the antigen in the hand eczema of nickel allergy. Contact Dermatitis. 1975;1(3):136-141.
Kaaber K, Veien NK, Tjell JC. Low nickel diet in the treatment of patients with chronic nickel dermatitis. Br J Dermatol. 1978;98(2):197-201.
Katta R, Schlichte M. Diet and dermatitis: food triggers. J Clin Aesthet Dermatol. 2014;7(3):30-36.
Özkaya E, Erdem Y, Aydoğdu IH, Sirkeci EG. Allergic Contact Dermatitis of the Hands: A Retrospective Cohort Study From Turkey Between 1996 and 2021. Contact Dermatitis. 2026;[Epub ahead of print].
Picarelli A, Di Tola M, Vallecoccia A, et al. Oral Mucosa Patch Test: A New Tool to Recognize and Study the Adverse Effects of Dietary Nickel Exposure. Biol Trace Elem Res. 2010;139(2):151-159.
Veien NK, Kaaber K. Nickel, cobalt and chromium sensitivity in patients with pompholyx (dyshidrotic eczema). Contact Dermatitis. 1979;5(6):371-374.
Veien NK, Hattel T, Laurberg G. Low nickel diet: an open, prospective trial. J Am Acad Dermatol. 1993;29(6):1002-1007.
Zirwas MJ, Molenda MA. Dietary Nickel as a Cause of Systemic Contact Dermatitis. J Clin Aesthet Dermatol. 2009;2(6):39-43.