What Is the Low Nickel Diet? A Doctor's Guide to the Diet That Healed 80% of Patients
What Is the Low Nickel Diet? A Doctor's Guide to the Diet That Healed 80% of Patients
In my last post, I explained what Systemic Nickel Allergy Syndrome (SNAS) is and why it causes so many mysterious symptoms. Now let's talk about what to actually do about it.
The answer, for most patients, is the low nickel diet — and the research behind it is remarkably compelling.
The Results Speak for Themselves
This isn't a fad diet. The clinical evidence is strong:
Over 80% of patients with chronic, allergic-like dermatitis who tested positive for nickel allergy achieved complete or near-complete recovery simply by switching to a low nickel diet (Antico & Soana, 2015).
For patients with gut-based nickel allergy (diagnosed via the oral mucosa patch test), 98.1% saw improvement in their intestinal and extra-intestinal symptoms after just two months (Picarelli et al., 2010).
In women with endometriosis and IBS-like symptoms who tested positive for nickel sensitivity, three months on the diet led to statistically significant reductions in GI pain, chronic fatigue, and chronic pelvic pain (Borghini et al., 2020).
And in IBS patients with nickel allergy, the diet not only improved symptoms but also helped address the underlying intestinal permeability — the "leaky gut" caused by the metal (Rizzi et al., 2017).
Where Does Dietary Nickel Come From?
For the general population, the daily diet is the primary source of nickel exposure (Sharma, 2013). Nickel is a natural element in the earth's crust, and plants absorb it through their roots from soil and water. This means plant tissues contain significantly more nickel than animal tissues (Lusi et al., 2015).
Processing and cooking multiply the problem. Cooking acidic foods like tomato sauce in stainless steel pots causes nickel to leach directly into your food (Zirwas & Molenda, 2009).
The Major Food Categories to Limit
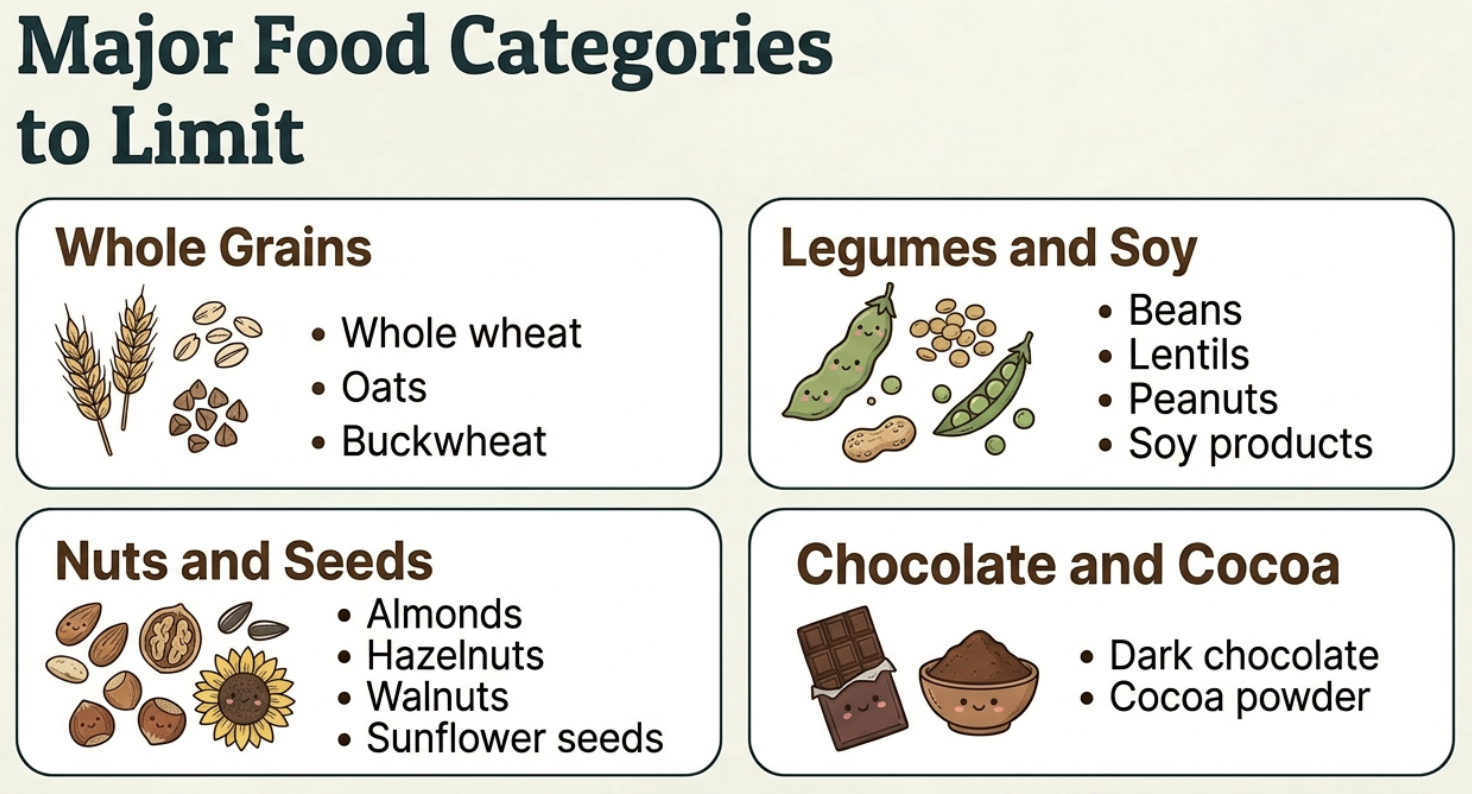
High nickel food to avoid: nuts, seed, legumes, soy, chocolate, whole grains, oats
The low nickel diet asks you to reduce or avoid foods that are "hyper-accumulators" — meaning they concentrate nickel far above average levels:
Whole grains: Whole wheat, oats, buckwheat.
Legumes and soy: Beans, lentils, peas, peanuts, and soy products.
Nuts and seeds: Almonds, hazelnuts, walnuts, sunflower seeds.
Chocolate and cocoa: Especially dark chocolate and cocoa powder.
I know — every single one of those is a "health food." That's the paradox of SNAS. But here's the critical thing to understand: you don't have to eliminate everything.
The 150 Microgram Threshold
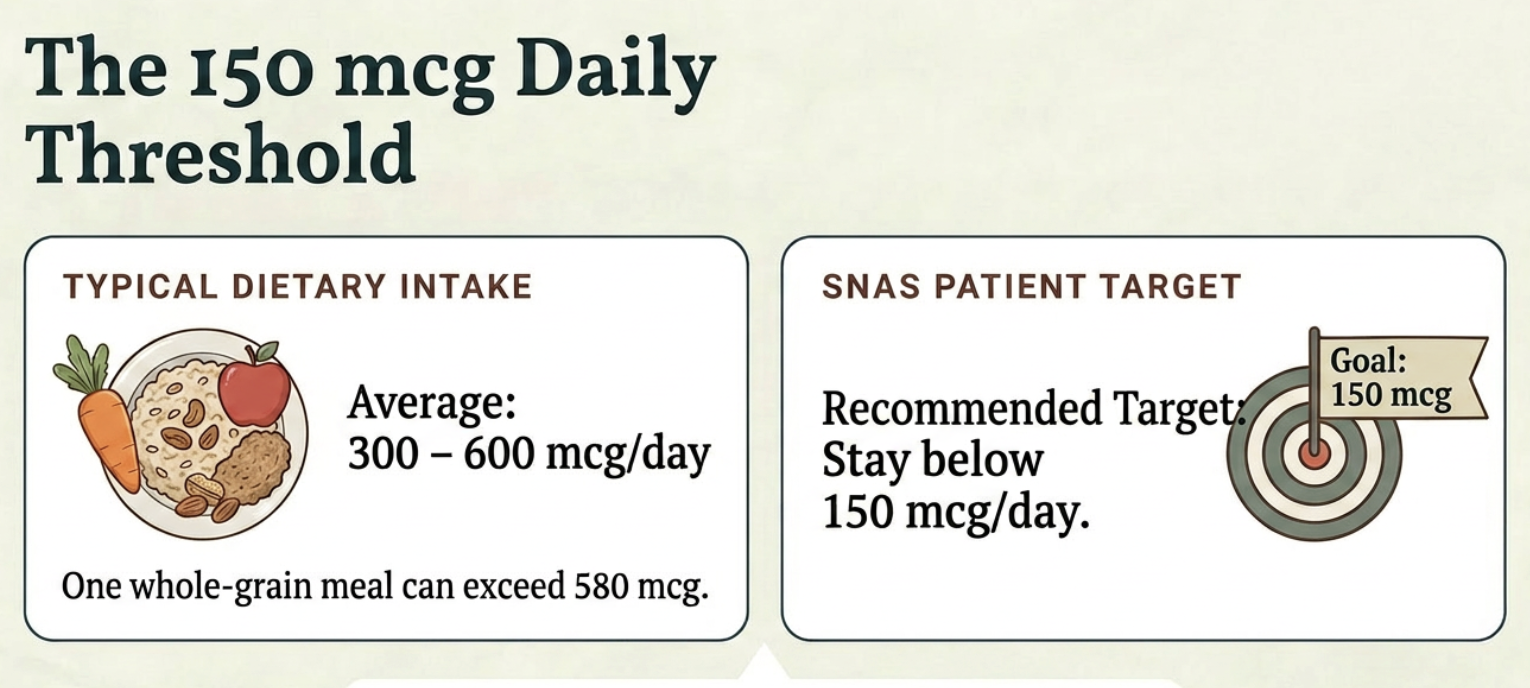
Research shows keeping nickel below 150 mcg a day reduces symptoms within 3 months
A typical Western diet contains between 300 and 600 micrograms (mcg) of nickel per day. A single "healthy" meal of oatmeal, nuts, and whole wheat bread can exceed 580 mcg (Zirwas & Molenda, 2009).
But research shows that only about 1% of sensitized patients react at typical dietary levels (Bergman et al., 2016). The recommended target for SNAS patients is to keep daily dietary nickel intake below 150 mcg per day (Mislankar & Zirwas, 2013).
You don't need a zero-nickel diet. That's impossible — nickel is the fifth most common element on Earth. You just need to stay under your threshold.
The Nickel Bucket: A Simple Tracking System
Think of your daily nickel tolerance like a bucket. Every food you eat adds water to the bucket. You're fine as long as the bucket doesn't overflow.
The points system makes this easy: 10 mcg of nickel = 1 point. Your goal is to stay under 15 points per day (Mislankar & Zirwas, 2013).
This means you can fit some higher-nickel foods into your day, as long as the rest of your meals are low. It's about managing your total load — not perfection.
How Long Until You Feel Better?
The strict elimination phase typically lasts 4 to 8 weeks, and up to 3 months (Katta & Schlichte, 2014; Rizzi et al., 2017). Most patients begin to see significant improvement within this window.
Once symptoms resolve, you move into a reintroduction phase where you gradually test your personal tolerance — finding the line between "fine" and "flare."
In some clinical settings, doctors also offer oral hyposensitization (sometimes called "nickel vaccination"), where micro-doses of oral nickel are given over months to build immune tolerance (Minelli et al., 2010). This can allow patients to eventually reintroduce more foods.
Two Quick Wins That Cost You Nothing
Take Vitamin C with meals. Vitamin C binds to nickel in your gut, reducing how much enters your bloodstream. It's one of the only supplements actively recommended on the low nickel diet (Solomons et al., 1982; Zirwas & Molenda, 2009).
Run your tap water in the morning. Nickel from water on an empty stomach absorbs at a rate 40 times higher than nickel consumed in food (Solomons et al., 1982). Nickel leaches from plumbing overnight, so running your faucet for 2 to 3 minutes before drinking or making coffee can drastically reduce your exposure (Sharma, 2013).
Common Myths About the Low Nickel Diet
"I have to eat zero nickel." Impossible. The goal is LOW, not zero. Stay under your threshold.
"Nickel content is always the same in every food." It varies wildly depending on soil, season, and farming methods. Food lists are estimates — useful guides, not absolute laws (Pizzutelli, 2011).
"My problem must be gluten." Whole wheat is naturally high in nickel. Studies have shown that many patients diagnosed with "non-celiac wheat sensitivity" actually have a systemic nickel allergy — they're reacting to the metal, not the gluten protein (D'Alcamo et al., 2017).
Your Next Step
Ready to start? Download my free Nickel Food List — it breaks down which foods are high, moderate, and low in nickel so you can start making swaps today.
Download the Free Nickel Food List →
Next in this series: I'll show you the shocking connection between IBS and nickel allergy — and why the low FODMAP diet only partially works for some patients.
References
Antico A, Soana R. Nickel sensitization and dietary nickel are a substantial cause of symptoms provocation in patients with chronic allergic-like dermatitis syndromes. Allergy Rhinol (Providence). 2015;6(1):e56-e63.
Bergman D, Goldenberg A, Rundle C, Jacob SE. Low Nickel Diet: A Patient-Centered Review. J Clin Exp Dermatol Res. 2016;7:355.
Borghini R, Porpora MG, Casale R, et al. Irritable Bowel Syndrome-Like Disorders in Endometriosis: Prevalence of Nickel Sensitivity and Effects of a Low-Nickel Diet. An Open-Label Pilot Study. Nutrients. 2020;12(2):341.
D'Alcamo A, Mansueto P, Soresi M, et al. Contact Dermatitis Due to Nickel Allergy in Patients Suffering from Non-Celiac Wheat Sensitivity. Nutrients. 2017;9(2):103.
Di Gioacchino M, Ricciardi L, De Pità O, et al. Nickel oral hyposensitization in patients with systemic nickel allergy syndrome. Ann Med. 2014;46(1):31-37.
Katta R, Schlichte M. Diet and dermatitis: food triggers. J Clin Aesthet Dermatol. 2014;7(3):30-36.
Lusi EA, Di Ciommo VM, Patrissi T, Guarascio P. High Prevalence of Nickel Allergy in an Overweight Female Population: A Pilot Observational Analysis. PLoS One. 2015;10(3):e0123265.
Minelli M, Schiavino D, Musca F, et al. Oral hyposensitization to nickel induces clinical improvement and a decrease in TH1 and TH2 cytokines in patients with systemic nickel allergy syndrome. Int J Immunopathol Pharmacol. 2010;23(1):193-201.
Mislankar M, Zirwas MJ. Low-nickel diet scoring system for systemic nickel allergy. Dermatitis. 2013;24(4):190-195.
Picarelli A, Di Tola M, Vallecoccia A, et al. Oral Mucosa Patch Test: A New Tool to Recognize and Study the Adverse Effects of Dietary Nickel Exposure. Biol Trace Elem Res. 2010;139(2):151-159.
Pizzutelli S. Systemic nickel hypersensitivity and diet: myth or reality? Eur Ann Allergy Clin Immunol. 2011;43(1):5-18.
Rizzi A, Nucera E, Laterza L, et al. Irritable Bowel Syndrome and Nickel Allergy: What Is the Role of the Low Nickel Diet? J Neurogastroenterol Motil. 2017;23(1):101-108.
Sharma AD. Low nickel diet in dermatology. Indian J Dermatol. 2013;58(3):240.
Solomons NW, Viteri F, Shuler TR, Nielsen FH. Bioavailability of nickel in man: effects of foods and chemically-defined dietary constituents on the absorption of inorganic nickel. J Nutr. 1982;112(1):39-50.
Zirwas MJ, Molenda MA. Dietary Nickel as a Cause of Systemic Contact Dermatitis. J Clin Aesthet Dermatol. 2009;2(6):39-43.