Fiber on a Low Nickel Diet: Essential or Optional for SNAS, MCAS & Histamine Intolerance?
If you're living with Systemic Nickel Allergy Syndrome (SNAS), Mast Cell Activation Syndrome (MCAS), or Histamine Intolerance (HIT), you've probably heard two completely opposite things about fiber. Some practitioners say you need 25–38 grams a day for gut health. Others — especially in the carnivore and low-histamine communities — say fiber is unnecessary or even harmful.
So which is it?
After reviewing 29 peer-reviewed studies, here's where the evidence actually lands: fiber is beneficial, but it is not biochemically essential. Whether you should add it to your low-nickel diet depends entirely on your individual situation — your symptoms, your eating pattern, and whether your gut can tolerate it.
This article walks through both sides of the argument with full citations so you can make an informed decision with your healthcare provider.
What Fiber Does in the Body
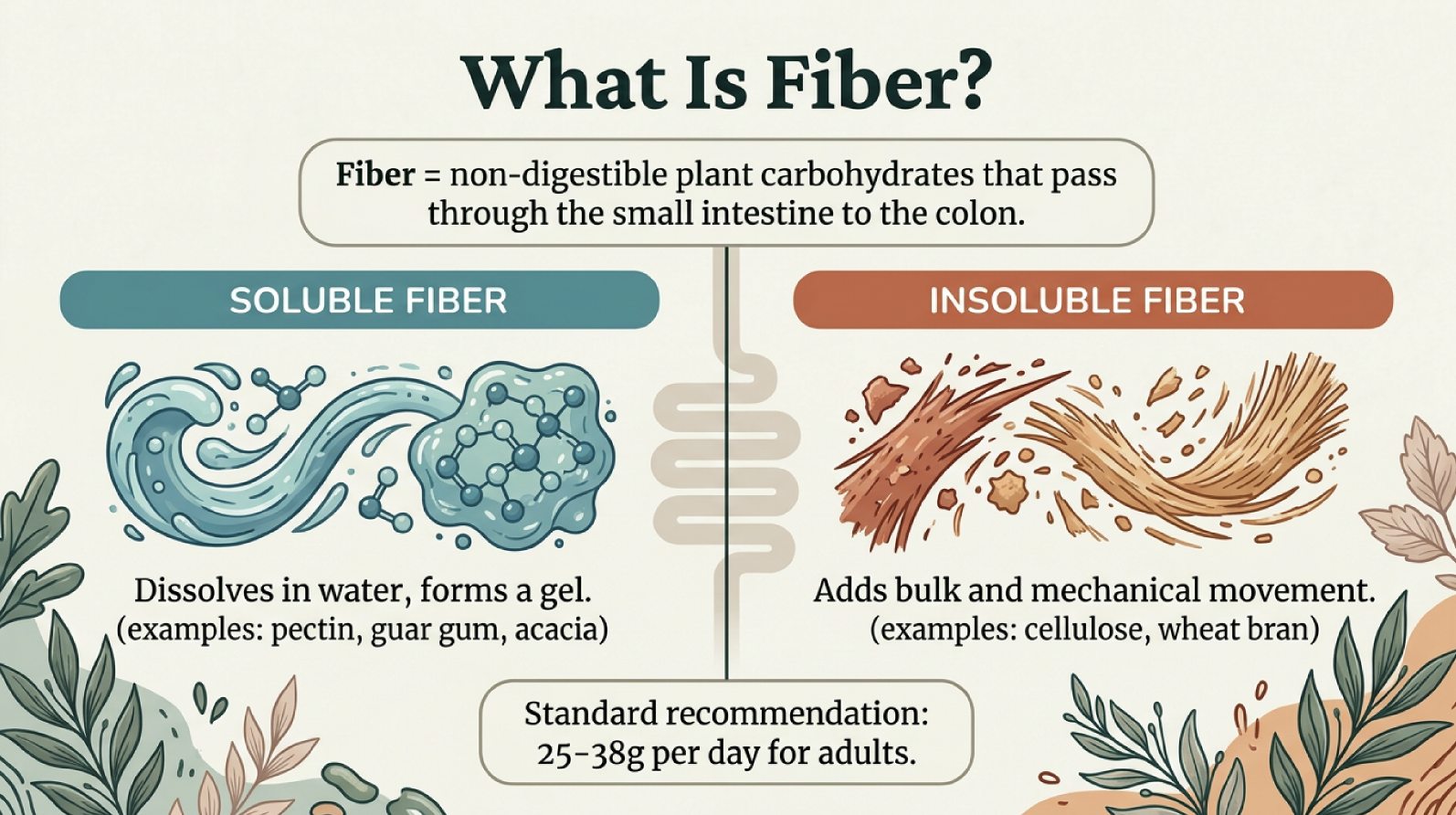
Fiber is a non-digestible plant carbohydrate that passes through the small intestine and arrives in the colon, where bacteria ferment it into short-chain fatty acids (SCFAs) — most importantly, butyrate.
Butyrate is the primary fuel for colonocytes (colon cells) and has been shown to stabilize mast cells by inhibiting MAPK, NF-κB, and AP-1 signaling pathways, reducing degranulation and histamine release (Folkerts et al., 2018, Frontiers in Immunology). It also strengthens the colonic barrier by upregulating tight junction proteins claudin-1, ZO-1, and occludin (Peng et al., 2009; Wang et al., 2012).
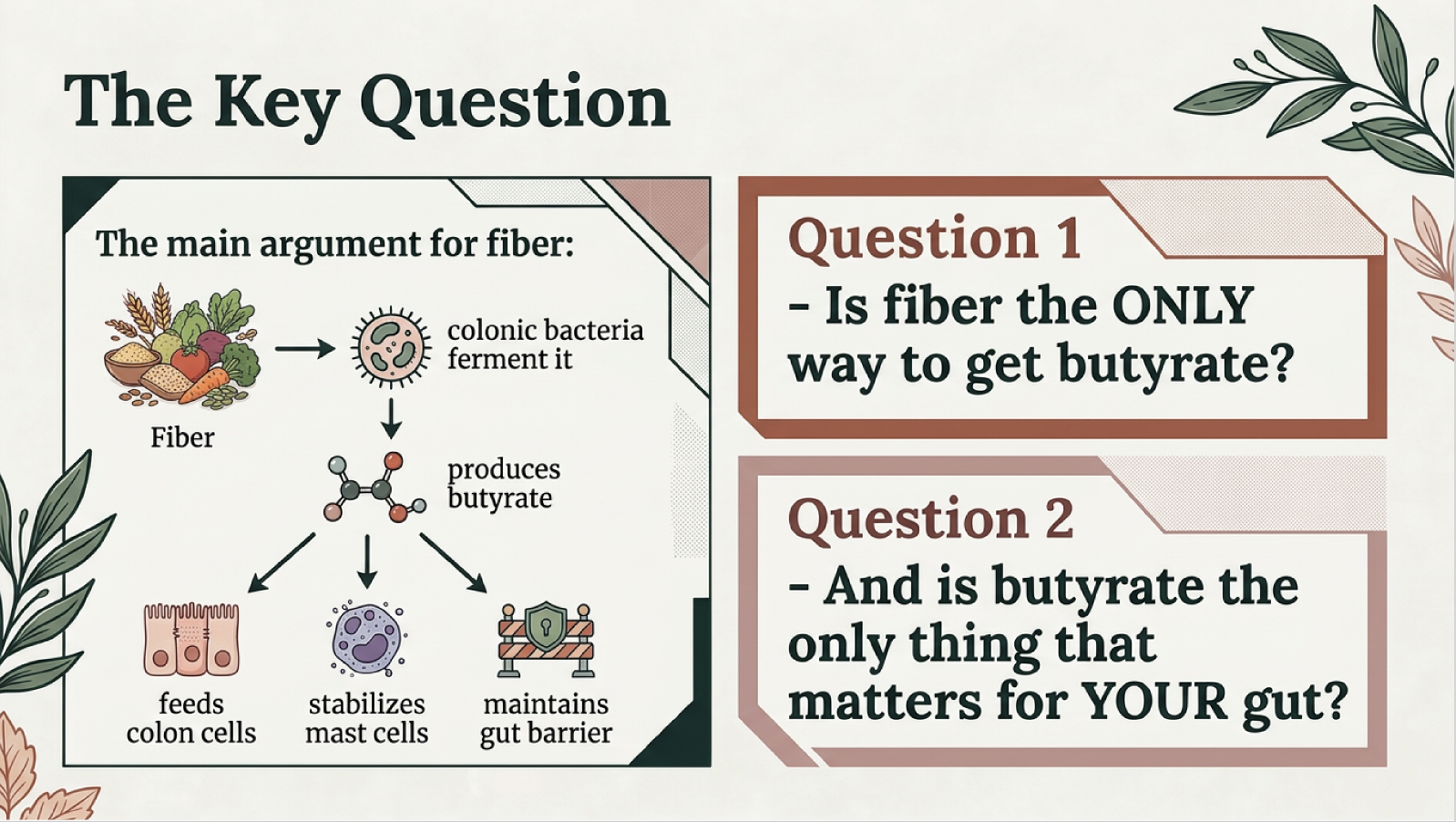
Is fiber the only way to get butyrate for the colon? no
For the general population, these are significant, well-documented benefits.
Why Fiber Is Complicated for SNAS, MCAS & HIT Patients
Here's the problem: the foods highest in fiber are also the foods highest in nickel.
The daily nickel target for SNAS patients is generally considered to be under 150 mcg total (EFSA, 2020). A single bowl of oatmeal can exceed that in one sitting.
This is the nickel-fiber paradox — and it's why so many people on a low-nickel diet end up eating very little fiber by default.
The Two Neighborhoods of Your Gut
You need to consider where your main concerns are so you know where to target with your strategy.
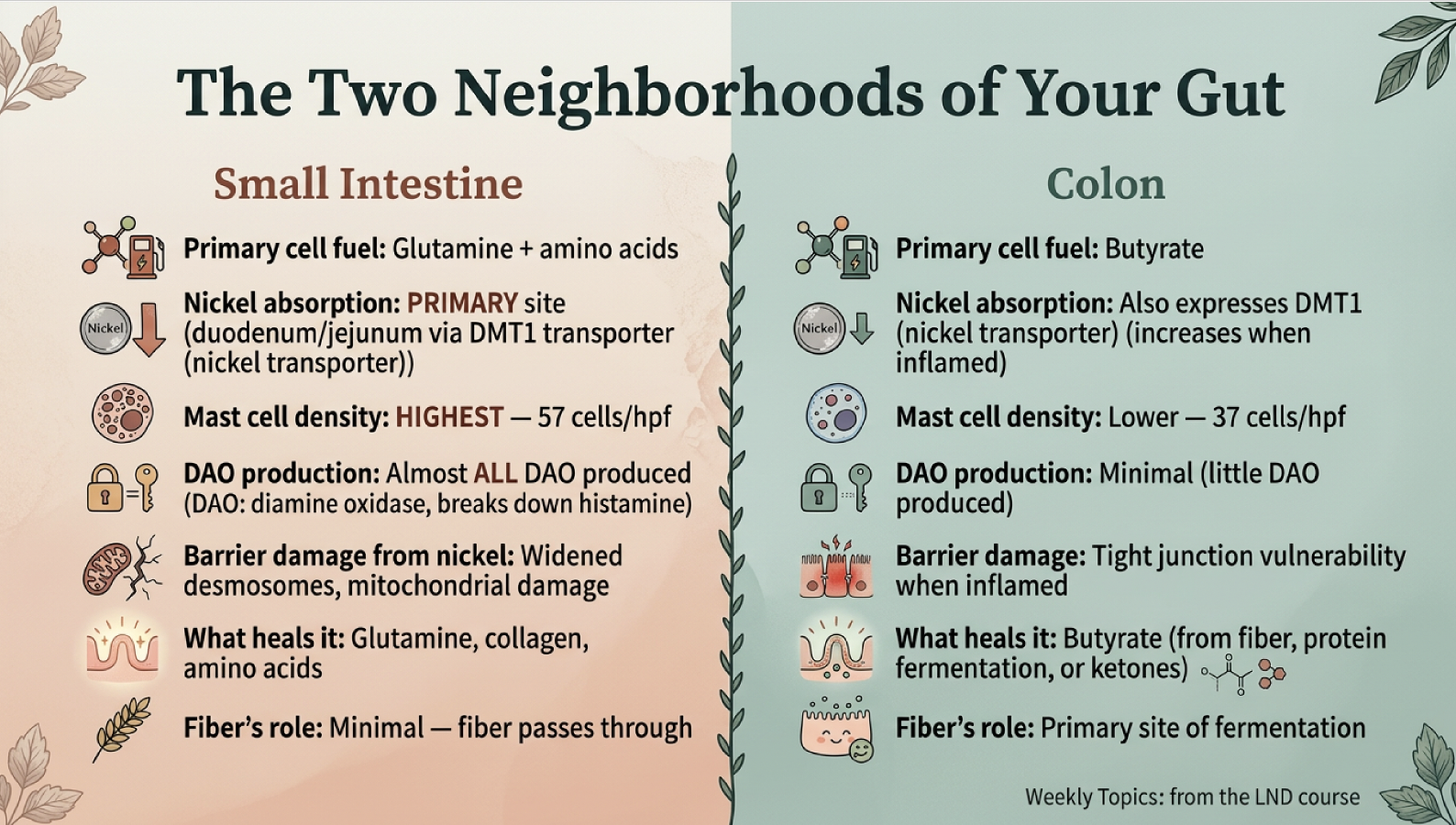
One of the most important and underappreciated concepts in this discussion is that your gut has two fundamentally different regions with different fuel needs.
The small intestine is where most nickel is absorbed (via the DMT1 transporter in the duodenum and jejunum), where mast cell density is highest (57 cells per high-power field vs. 37 in the colon), and where almost all DAO — the enzyme that breaks down histamine — is produced. The small intestine runs on glutamine and amino acids, not butyrate.
The colon is where fiber is fermented into butyrate. But the colon is not a "safe zone" — it also expresses DMT1 nickel transporters at levels comparable to the duodenum, and those transporters increase when the colon is inflamed (Sharma et al., 2020, Biological Trace Element Research).
This means both neighborhoods need protection — but with different fuel. The small intestine needs glutamine (from meat, collagen, broth). The colon needs butyrate (from fiber fermentation, protein fermentation, or ketones).
How to Get Fiber on a Low-Nickel Diet
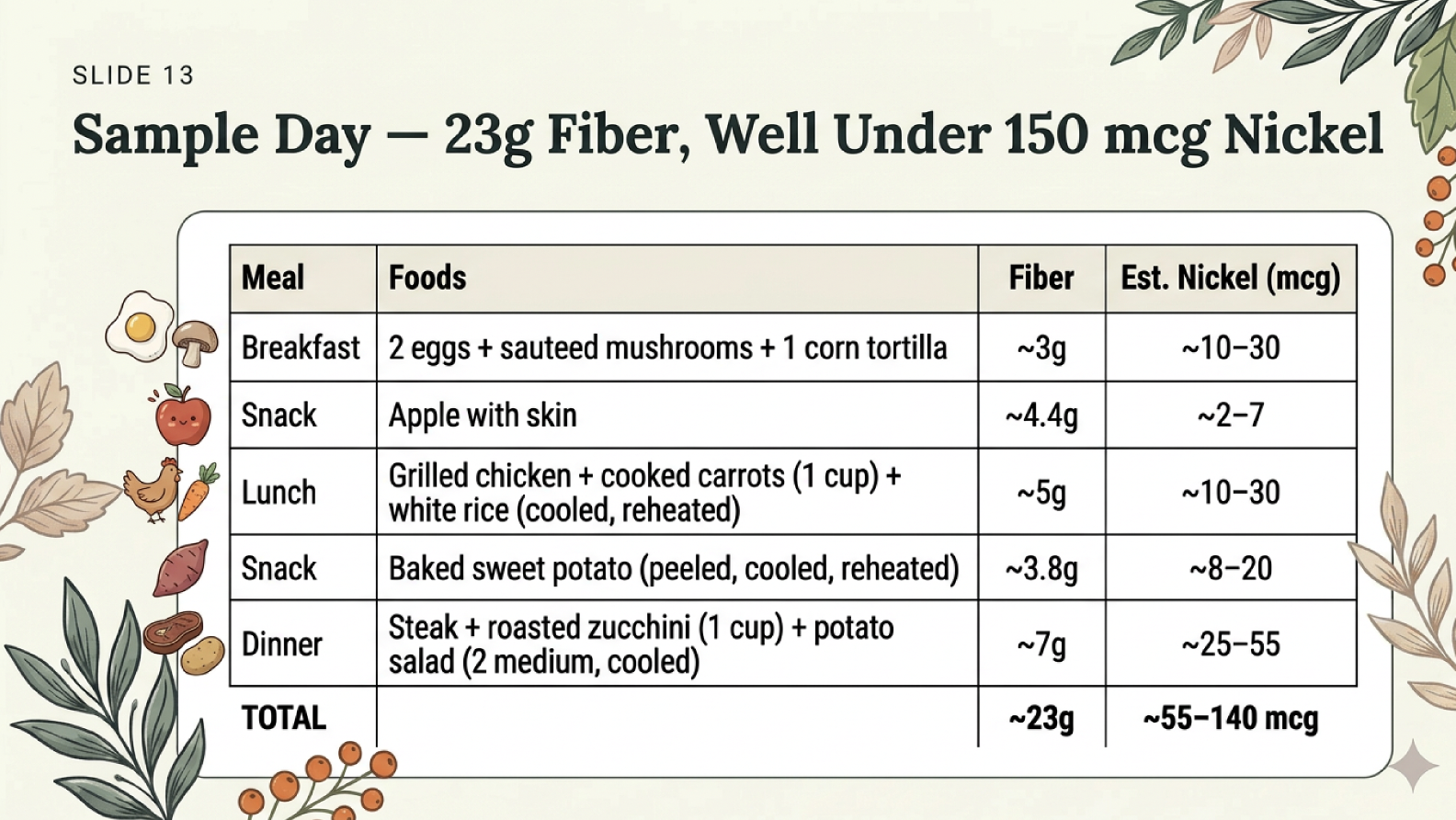
It IS possible to get meaningful fiber while staying under your nickel target. The key is choosing the right foods.
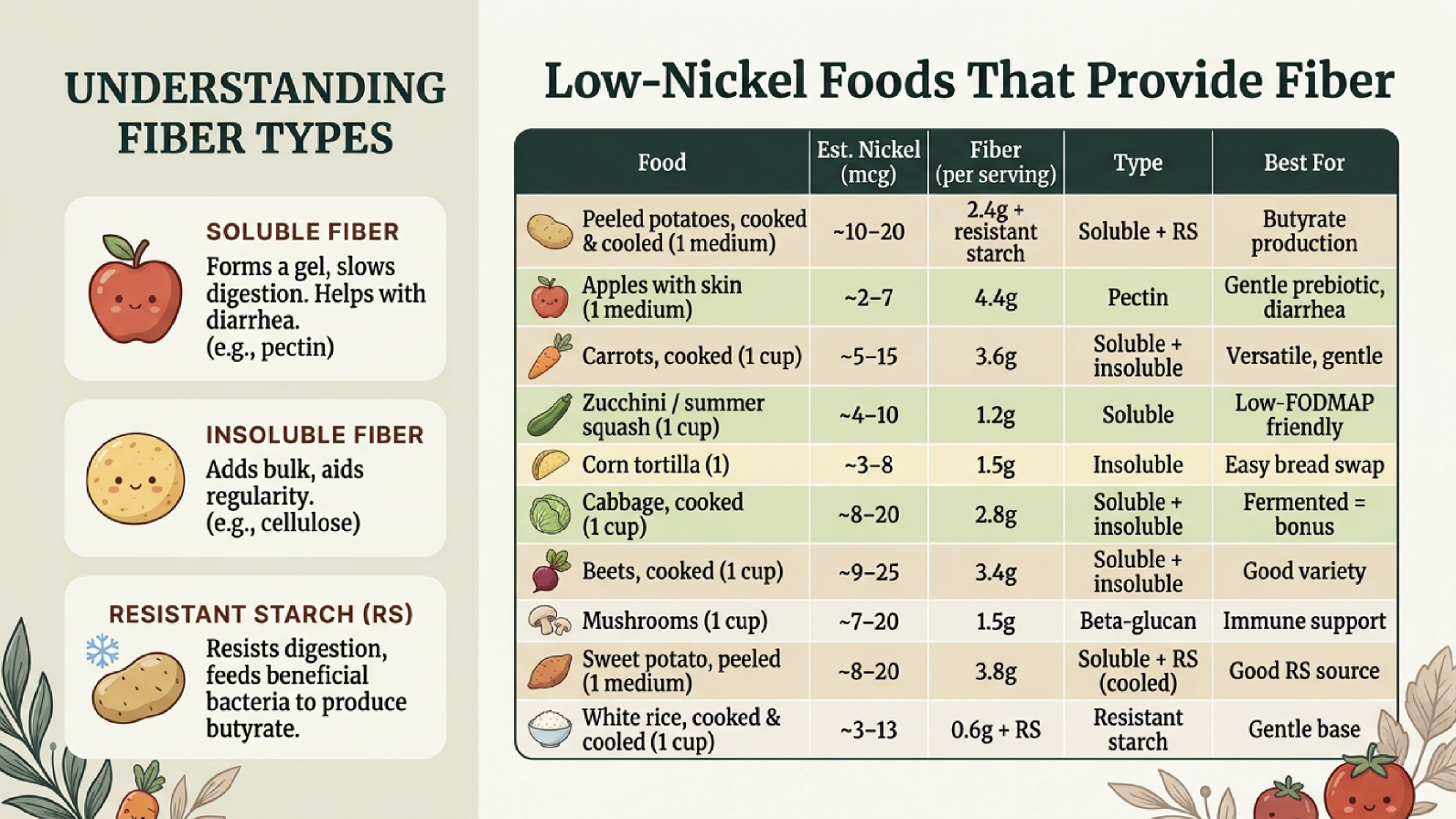
A full day using these foods can yield approximately 23 grams of fiber on an estimated 55–140 mcg of nickel — well within the daily target.
Get your fiber on a low nickel diet
The cooked-and-cooled technique is especially valuable: when you cook potatoes or rice and then refrigerate them, the starch retrogrades into resistant starch, which is fermented into butyrate in the colon. You can reheat and much of the benefit remains.
Why Some People Thrive Without Fiber
You may not need fiber to accomplish your health goals.
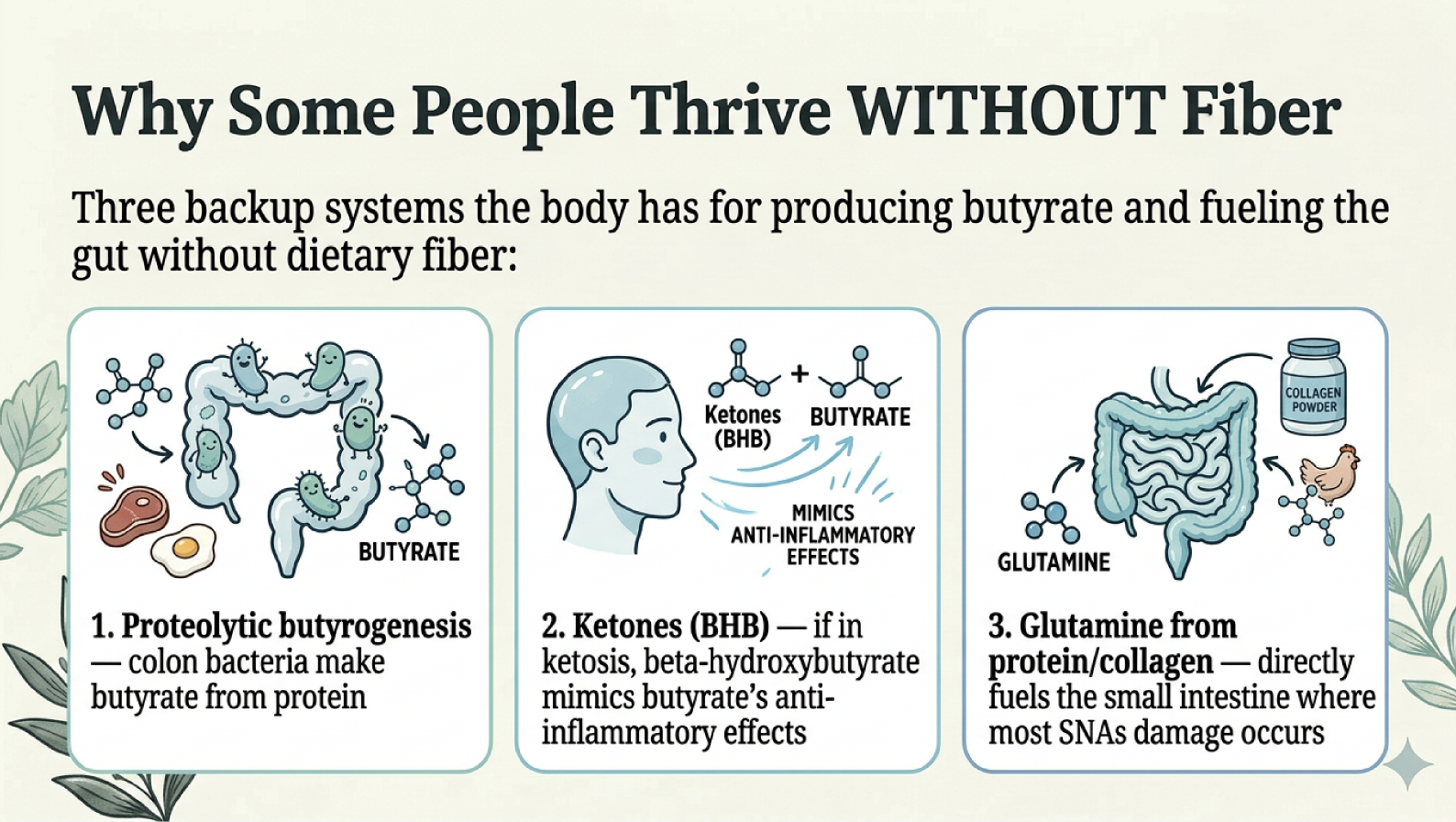
Fiber is not classified as an essential nutrient. It has no deficiency syndrome — no acute clinical failure occurs in its absence if the diet is otherwise complete. And your body has backup systems for producing butyrate without fiber.
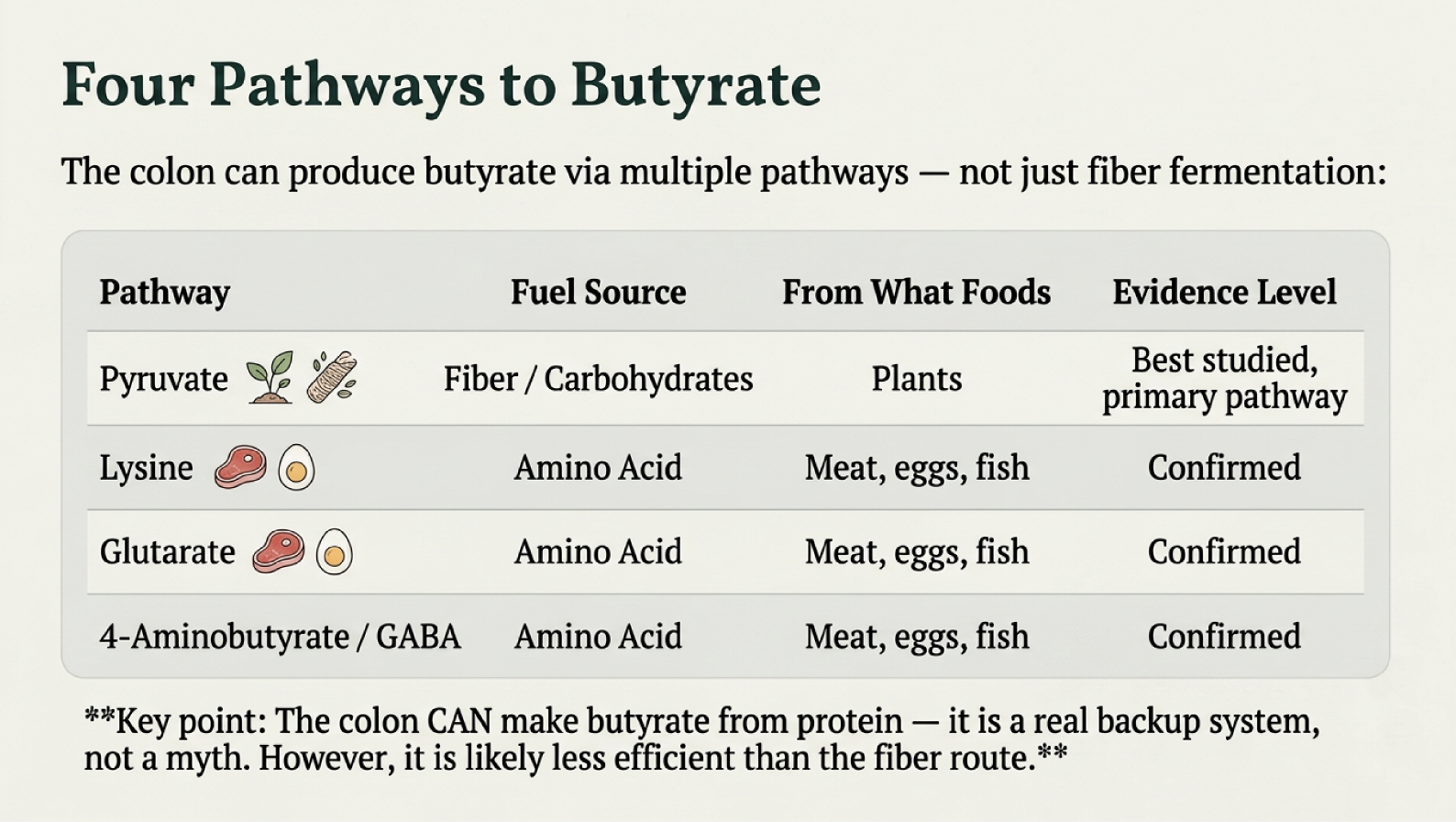
Proteolytic butyrogenesis: Your colon bacteria have four confirmed pathways to produce butyrate, and three of them use amino acids from protein — lysine, glutarate, and 4-aminobutyrate (Vital et al., 2014, mBio). This means a protein-rich diet does provide some colonic butyrate, though likely less efficiently than the fiber route.
Beta-hydroxybutyrate (BHB): During ketosis, the liver produces BHB, which activates the same receptor as butyrate (GPR109A) and inhibits the NLRP3 inflammasome — a major driver of systemic inflammation and mast cell activation (Youm et al., 2015, Nature Medicine). However, this benefit requires ketogenic-level carbohydrate restriction (<20–50g/day). Most people eating a moderate low-nickel diet with potatoes and rice are NOT in ketosis.
Glutamine: The small intestine — where most SNAS damage occurs — runs on glutamine, not butyrate. Meat, bone broth, collagen, and eggs provide glutamine directly to the cells most under attack from nickel.
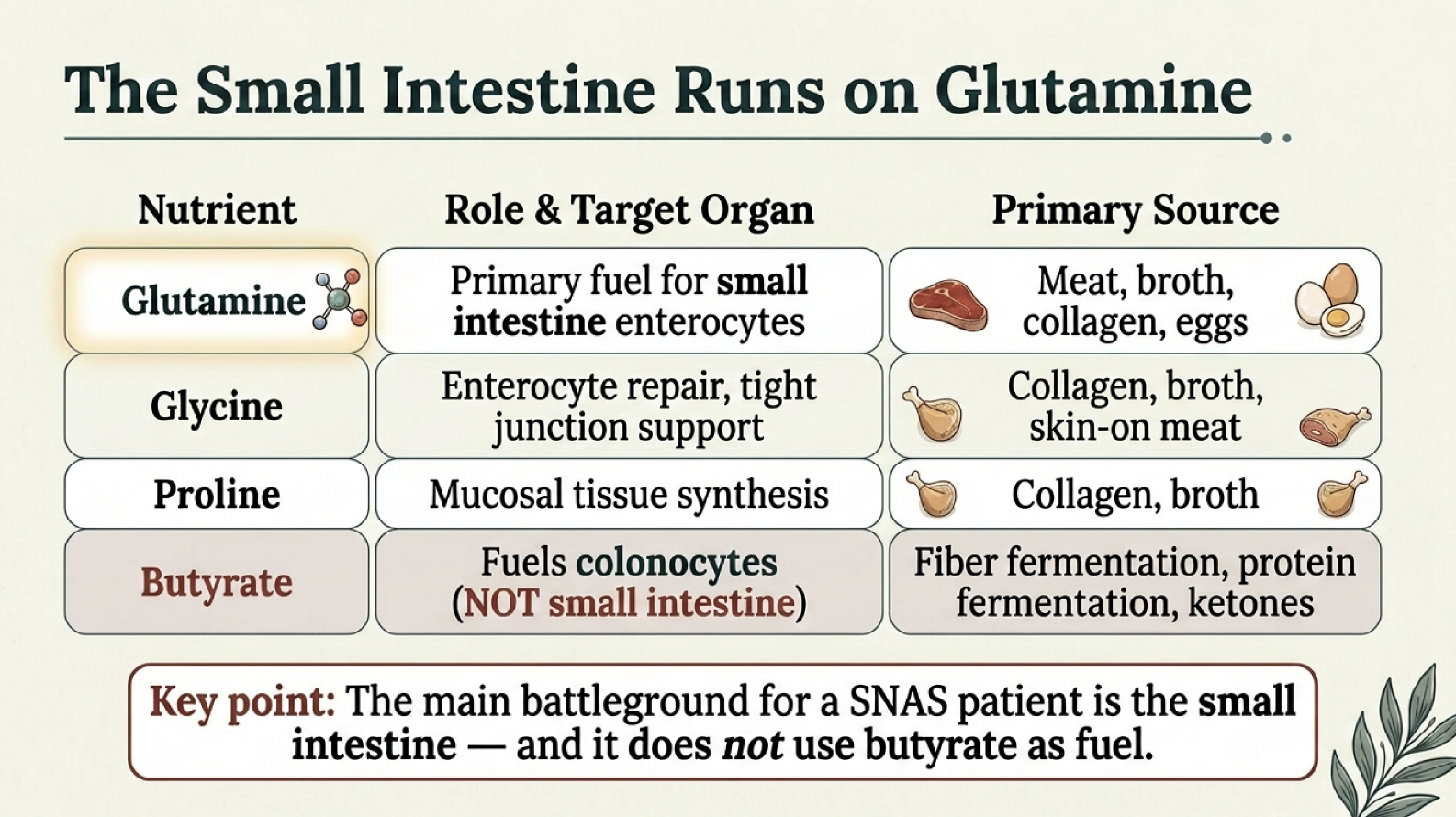
Small intestinal health needs glutamine, not butyrate
The SIBO Complication
If fiber consistently makes you feel worse — bloating, gas, pain, histamine symptoms — the problem may not be the fiber itself. It may be Small Intestinal Bacterial Overgrowth (SIBO), where bacteria have colonized the small intestine where they don't belong. Feeding fermentable fiber to misplaced bacteria produces gas and histamine in the wrong location.
One notable exception: partially hydrolyzed guar gum (PHGG) combined with rifaximin improved SIBO eradication from 62% to 87% in a clinical trial (Furnari et al., 2010, Alimentary Pharmacology & Therapeutics). If you're working with your doctor on SIBO, ask about this combination.
A Decision Framework
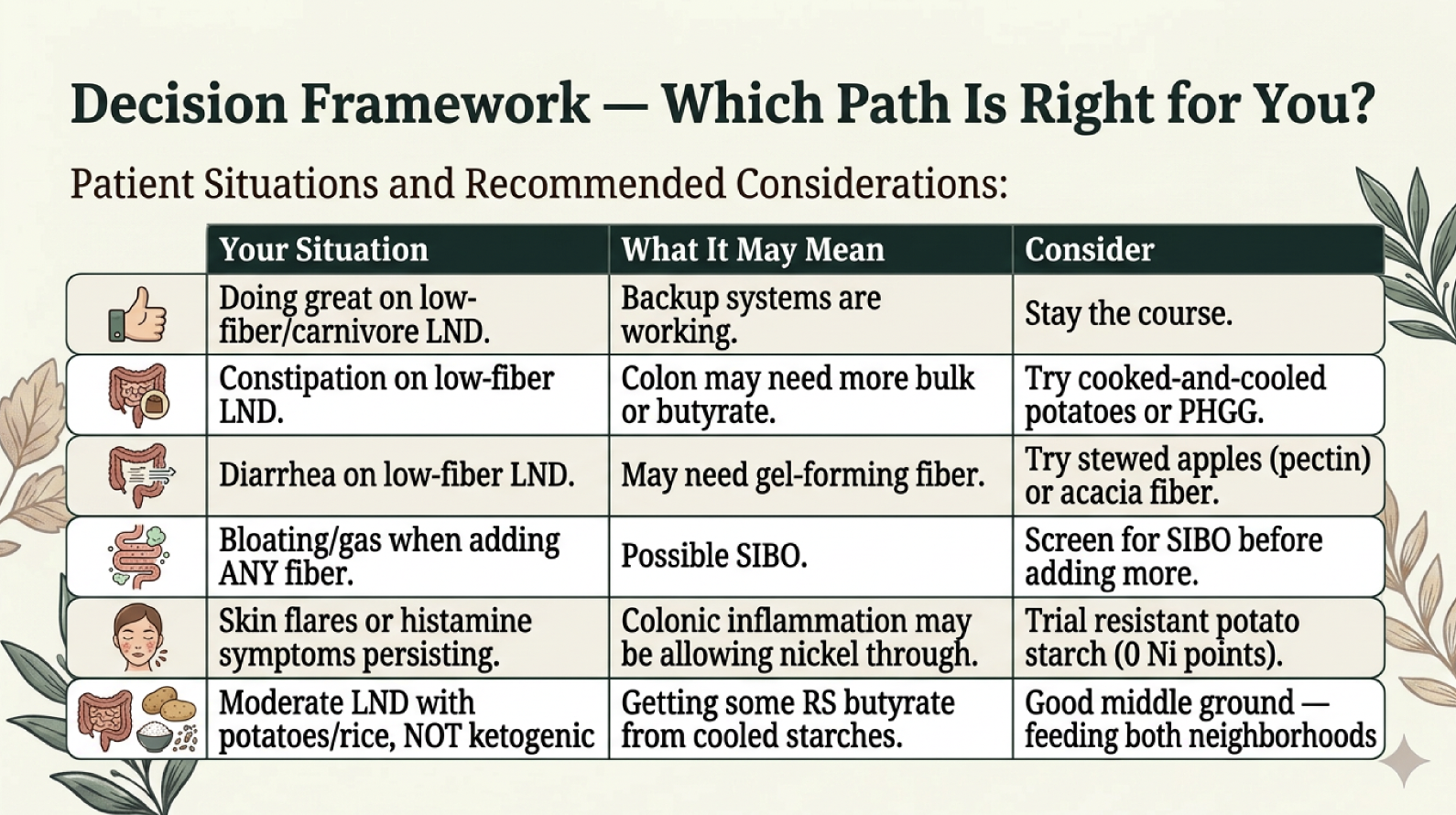
How to decide what your fiber strategy should be.
The Bottom Line
Fiber is a beneficial tool — not a biological requirement. Your gut has two neighborhoods with different needs, and understanding which one is most under stress helps you make a smarter choice.
If you're thriving without fiber, you don't need to panic. If you're struggling, there are safe, low-nickel options to try — one at a time, starting slow.
Neither path is wrong. The right path is the one that works for YOUR body.
This article is for educational purposes only and is not intended as medical advice. Always consult your healthcare provider before making changes to your diet or treatment plan.
References
Folkerts J et al. Effect of dietary fiber and metabolites on mast cell activation. Front Immunol. 2018;9:1067.
Vital M et al. Revealing the bacterial butyrate synthesis pathways. mBio. 2014;5(2):e00889-14.
Youm YH et al. BHB blocks NLRP3 inflammasome-mediated inflammatory disease. Nat Med. 2015;21(3):263-269.
Peng L et al. Butyrate enhances intestinal barrier via AMPK in Caco-2 cells. J Nutr. 2009;139(9):1619-1625.
Wang HB et al. Butyrate enhances barrier function via claudin-1. Dig Dis Sci. 2012;57(12):3126-3135.
Furnari M et al. Rifaximin + PHGG is more effective in eradicating SIBO. Aliment Pharmacol Ther. 2010;32(8):1000-1006.
Solomons NW et al. Bioavailability of nickel in man. J Nutr. 1982;112(1):39-50.
EFSA Panel on Contaminants. Nickel in food and drinking water. EFSA J. 2020;18(11):e06268.
Sharma J et al. Increased DMT1 expression in ulcerative colitis colon. Biol Trace Elem Res. 2020;195(1):74-81.
Maintz L, Novak N. Histamine and histamine intolerance. Am J Clin Nutr. 2007;85(5):1185-1196.